
Fever in a Splenectomized Patient
Authors: Thomas Rushton M.D., FACP, FIDSA, FSHEA
INTRODUCTION
The spleen is the largest lymph node in the body, and its loss is expected to weaken the immunity of its host leading to an increased incidence, and severity, of infection. When life-threatening, these infections are termed either overwhelming postsplenectomy infections (OPSI) or postsplenectomy sepsis. Even with preventative measures, death remains a real threat. It is incumbent upon the physician to educate the patient, providing specific advice about when to seek care and what to do while awaiting care. Securing the diagnosis and administering appropriate therapies and supportive care will increase the likelihood of the survival of the patient. Determining possible exposures is very important as travel and animal bites are common themes when the causative organism is finally determined.
The approach to a patient without a spleen must consider the underlying condition leading to splenectomy, preventative measures, and possible exposures (19,24).

Epidemiology
A spleen is most commonly removed because of trauma where extensive damage and bleeding necessitates its removal. A splenectomy may need to be performed due to iatrogenic misadventure during a surgical procedure. During open gastric bypass, for example, the splenic vasculature might become compromised necessitating removal of the spleen.
Splenic dysfunction may be caused by immunological or hemolytic etiologies (e.g., autoimmune hemolytic anemia, idiopathic thrombocytopenic purpura), hypersplenism (thalassemia, type 1 Gaucher’s disease), or malignancy (Hodgkin’s disease, ovarian carcinoma) (27). Celiac sprue is a leading cause of asymptomatic hyposplenism (12).
There are a number of conditions (Table 1) that produce varying degrees of functional hyposplenism. Sickle cell anemias, hemophilia and other hematologic disorders often lead to splenic dysfunction. Autoimmune disorders, such as biliary cirrhosis, chronic active hepatitis, rheumatoid arthritis, systemic lupus erythematosis, idiopathic vasculitides, inflammatory bowel disease and others, may be associated with loss of splenic function (10,11).
Amyloidosis and sarcoidosis, which infiltrate tissue, can damage the spleen significantly. Antigen-antibody complexes may alter blood flow or cause infarctions within the splenic tissue. Treatment of the underlying disorder frequently mitigates splenic dysfunction.
The incidence of infection is highest during the first through second year after splenectomy and decreasing thereafter. Approximately one of four patients will develop a significant infection in their lifetime. If the spleen has traumatically ruptured during its removal, splenic fragments may seed the peritoneal cavity, or less likely, the thorax (2).
Microbiology
The most fulminant infections in OPSI occur with encapsulated bacteria, including Streptococcus pneumoniae, Haemophilus influenzae type b and possibly Neisseria meningitides (Table 2). As newer bacteria are discovered and identified, some will be uniquely associated with asplenic patients but will not necessarily be encapsulated. Other non-bacterial pathogens such as protozoa are also capable of producing significant sepsis. Fulminant viral infections, when they occur in the asplenic patient, probably relate more to an underlying malignancy such as lymphoma or chronic leukemia.
S. pneumoniae is implicated most commonly. Published studies have reported rates from forty to 100% of their isolates being identified as S. pneumoniae. Personal experience is commiserate with these findings with the additional reminder of the rapidity in which a patient may die with this infectious process. Multiple capsular oligosaccharides, used in serotyping, have been described. Virulence differs between serotypes (21). Resistance to penicillin, broader-spectrum cephalosporins and now fluoroquinolones make antibiotic recommendations more controversial. It is clear that host defense and reserve are the strongest predictors of survival as penicillin resistance, as currently reported, does not affect clinical outcome (20,34).
Haemophilus influenzae type b (Hib) has singularly become very uncommon in the United States, but remains common in other parts of the world. This is due in no small part to the introduction and successful administration of Haemophilus influenzae type b vaccine. More recently, other serotypes of encapsulated as well as other non-encapsulated H. influenzae strains are being isolated. There is no indication that they pose an increased threat in splenectomized patients as they are frequent colonizers of the respiratory tracts of humans. Generally, H. influenzae is a rare cause of infection in these patients (21). Resistance due to beta-lactamase formation is common but is readily countered by the use of antibiotics stable against this enzyme or the addition of an inhibitor to the beta-lactam antimicrobial agent.
Neisseria meningitidis causes devastating illness with septic shock associated with septicemia and meningtitis. Multi-organ dysfunction occurs with vascular compromise; if the adrenal glands are destroyed, the Waterhouse-Friderichsen syndrome may develop. Capsular polysaccharides include A, B, C types, X, Y and W-135. Beta-lactamase resistance is becoming more prevalent. Other choices such as trimethoprim-sulfamethoxazole or chloramphenicol are not to be recommended. Whether N. meningitidis is actually a greater threat in the asplenic or hyposplenic patient remains debatable. I share the opinion that asplenism does not greatly increase the risk for N. meningitidis infection. For all of these bacteria, the choice of antibiotic will need to be made on the basis of available route, tolerance, drug interactions and central nervous system penetration.
Capnocytophaga canis (formerly Dysgonic fermenter 2 (DF-2)) is a gram negative bacillus that inhabits the mouths of dogs. It is an especially dangerous organism in asplenic individuals where shock and progression to death can be quite rapid. A history of exposure to dogs and possible trauma needs to be elicited. A purpuric rash may develop, and the physical examination should be made carefully to assess for tissue trauma that might suggest a dog bite. The presence of such would argue against N. meningitides. If a bite wound is found, the site should be monitored for changes consistent with gangrene.
Bordetella holmesii, first recovered from an asplenic patient in 1983, causes septicemia, endocarditis and respiratory illness. In a report of 26 cases, 22 occurred in asplenic or hyposplenic patients (10). Infections are generally mild but antimicrobial therapy is recommended until further is known. Modes of transmission remain unknown and animal exposure has not been ruled out.
Salmonella species share an association with OPSI, but in most cases the infection reflects deficient cellular immunity due to the primary disease or its treatment. Sickle-cell anemia-associated splenic dysfunction, especially in afflicted children, has a strong correlation with Salmonella infections.
Babesia microtis, or cattle malaria, is usually contracted via the bite of a hard tick while traveling in an endemic area. Blood transfusions have also been implicated. A febrile illness occurs with myalgias, fatigue, hemolytic anemia and hemoglobinuria. In the splenectomized patient, the illness may range from moderate to severe, but most will survive. The highest concentration of cases has been found on offshore islands of the northeastern United States (Nantucket Island, Martha’s Vineyard, the eastern tip of Long Island) and Cape Cod. Cases have been reported from Wisconsin, Minnesota, Georgia, California and Mexico. Other Babesia species have been identified in Washington state and Missouri.
Splenectomy may predispose a traveler to more severe malaria (Plasmodia spp.) infection and reactivation of latent and subclinical infections. The spleen aids in the reduction of parasitemia but does so non-specifically by removal of pitted red blood cells and does not produce immunity against malaria. Patients returning from an endemic area should be questioned regarding anti-malarial prophylaxis and mosquito exposure, if they experience fever and associated sypmtoms. Asplenic patients should be counseled regarding the risk and inherent danger of malaria exposure and subsequent illness which may progress to death.
Pathogenesis
Humoral immunity is greatly affected by splenectomy. Organisms that require opsonization for their removal are associated with OPSI. IgG or complement fragments will attach to antigen-containing microbial surfaces. When marked in this fashion, the body’s macrophages and neutrophils are stimulated to phagocytosis of the microbe. An intracellular vesicle, or phagosome, forms and the invading organism is destroyed intracellulary.
Sepsis, the systemic inflammatory response syndrome with infection, is a complex response by the host to an invading micro-organism. It is characterized by upregulation of both pro-inflammatory and anti-inflammatory proteins, including interleukins and chemokines and alteration in the coagulation pathway (25). The recent introduction of recombinant human activated protein C (rhAPC) is the first direct treatment of severe sepsis and septic shock. While it appears that rhAPC does not have a direct effect on the dissolution of microvascular thrombosis, its addition to the severely septic patient does have an anti-inflammatory role. It remains a controversial component in sepsis treatment because of its propensity to bleeding, usually gastrointestinal and central nervous system; it is also costly.
An uncontrolled inflammatory response is now credited with the morbidity and mortality associated with bacterial meningitis. While once a recommendation for pediatric cases only, corticosteroid therapy, preferably dexamethasone, should be routinely administered to adult patients as well (9). The data are strongest in the presence of Streptococcus pneumoniae and some would not continue dexamethasone if the bacteria were different. Confounding and controversial issues surrounding corticosteroid administration occur in the face of both meningitis and septic shock and the decreased levels of antibiotic in the CSF. In the latter, this may be especially important with organisms that have increased resistance to beta-lactam antibiotics (31).
Corticosteroid therapy should be avoided if antibiotics have already been given, there is trauma to the head or the presence of a CSF shunt, or there is an allergy to corticosteroids.
Differential Diagnosis
In the appropriate clinical setting, OPSI must be given primary consideration, but other possibilities, although less likely, do exist (Table 3). When the criteria for SIRS are met, sepsis (again, progressing to severe sepsis and septic shock) should be treated empirically. The choice of antibiotic and time of the first dose are critical elements in ameliorating the effects of the invasive organism and preventing death.
In sickle cell anemia patients, painful crises can be accompanied by fever. In such cases, again, the patient should be worked up for underlying infection. Hemolysis may be associated with fever. However, acute chest pain syndrome presents with chest pain, fever, cough and abnormal oxygenation of blood and may be mistaken for pneumonia, pulmonary embolism, infarction of lung or other cardiopulmonary disaster.
Underlying malignancies or collagen vascular disorders may present with fever. A careful history will help disclose a drug-associated fever and should include prescription and over-the-counter medications and also herbal preparations and other nutritional supplements. Recreational, or “street” drugs, are also capable of producing drug-associated fevers.
Clinical Manifestations
OPSI is usually an acute process characterized by fever, chills, arthralgias/myalgias, headache and gastrointestinal complaints (Table 4). Obviously, there will be some variability depending on the duration and location of the infection (if there is one). The location and type of rash, if present, may be an aid to earlier diagnosis of the offending organism.
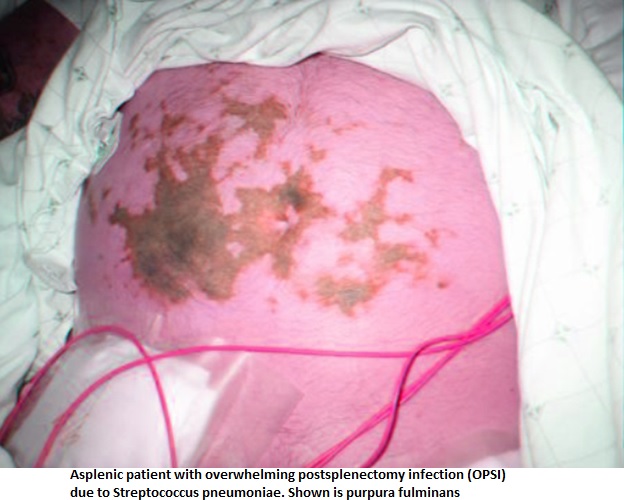
The patient may deteriorate quite rapidly. Cardiovascular collapse, disseminated intravascular coagulopathy, seizures, coma and gangrene (purpura fulminans) ![]() may be found. In such cases, amputation is frequently required.
may be found. In such cases, amputation is frequently required.
{kind=link}
{kind=link}
{kind=link}
Diagnosis (Table 5)
Laboratory Testing
Basic blood studies should include a complete chemistry profile that assesses renal and liver status. A complete blood count with differential is required to establish SIRS criteria. An arterial blood gas and lactic acid level is also needed and will help to determine perfusion status of the patient. Basic coagulation tests (INR and PTT, platelet count) may be followed up with a peripheral smear for hemolysis and platelet consumption. The smear may also disclose the presence of nucleated red blood cells (RBCs), anisocytosis and poikolocytosis (abnormal size and shape of RBCs), Howell-Jolly bodies (nuclear remnants) ![]() , Heinz bodies (denatured hemoglobin), and basophilic stippling. Such findings should confirm the absence of a functional spleen or lead one to suspect that it is absent, if this were not previously known. Fibrin and fibrin split products are required especially if drotrecogin is going to be administered.
, Heinz bodies (denatured hemoglobin), and basophilic stippling. Such findings should confirm the absence of a functional spleen or lead one to suspect that it is absent, if this were not previously known. Fibrin and fibrin split products are required especially if drotrecogin is going to be administered.
If the patient is profoundly neutropenic, a buffy coat differential should be performed. A thin blood smear is needed for more rapid diagnosis of Babesia or Plasmodium. In the former, a serological assay is available from the CDC (IgG IFA). A polymerase chain reaction test may be useful in detecting lower levels of parasitemia. A serological assay is also available for Plasmodium; in some parts of the world, rapid dip-stick tests for P. falciparum histidine-rich protein 2 (ParaSight F) and Plasmodium lactate dehydrogenase (OptiMal). There are limitations inherent in these tests as well as cross-reactivity potential.
A S. pneumoniae urine antigen is available. Because of colonization issues in the pediatric population, and the frequency in which this population remains positive, it is not recommended here. False positives do occur in the adult population (approximately 10-15% of patients with non-pneumococcal pneumonia), but as S. pneumoniae is the leading cause of infection in OPSI, it may prove quite helpful in providing a rapid diagnosis (16). As pneumonia may not be the presenting clinical scenario, this test should be obligatory in the initial work-up of the patient.
Cerebrospinal immunoassays are inferior to gram stain and culture (see below). With anticipated greater refinement, polymerase chain reaction analysis of CSF may one day be clinically useful in both rapid diagnosis and determination of etiology in gram stain and culture negative meningitis.
Cultures
At a minimum, two sets of blood cultures should be collected prior to initiating antimicrobial therapy. While it is common to include anaerobic blood cultures routinely, the overall yield is low except in presentations where anaerobes would be expected (e.g., visceral rupture or intra-abdominal abscess). Of paramount importance is that at least 10 ml of blood is inoculated into each bottle.
An abnormal urinalysis with leukocyte esterase, nitrites or pyuria should be sent for culture. Likewise, with patients with pneumonia, a good quality sputum specimen can provide rapid diagnosis by Gram staining and, generally, by the next day, culture. Poor quality specimens are not helpful. As S. pneumoniae is rapidly killed and other bacteria may quickly overgrow, any delay in the collection and/or processing of the specimen will preclude detection by culture.
If signs of meningeal irritation are present, cerebrospinal fluid should be collected for gram staining and culture.
Radiologic Imaging
Chest radiography, ultrasonography and CT scans are useful diagnostic tools and should be utilized on suspicion of the site of infection or to rule out a likely source, such as pneumonia. Other imaging modalities, such as nuclear scans, may be important adjunctive studies and may be considered with advice or discussion with a radiologist.
Generally, in the setting of possible meningitis, a lumbar puncture should not be delayed pending imaging of the central nervous system. If signs of brain shift (papilledema, focal neurologic signs (cranial nerve palsy excluded)) are present, the Glasgow Coma score is below 10, the patient is in a severe immunocompromised state (e.g., AIDS), or there are new onset seizures, then imaging should be obtained prior to the lumbar puncture.
Empiric Antibiotic Therapy (Prior to Definitive Diagnosis)
General Guidelines (Principles)
Resistant microbes are now the rule rather than the exception. Older or extensively used antibiotics are frequently less effective even for common and prevalent bacteria. A knowledge of resistance patterns, as they occur in the local community and in various parts of the hospital (e.g., the intensive care unit, a medical-surgical floor and neonatal unit), is requisite. Both local and state health departments and their epidemiologists and a hospital’s infection control program are invaluable resources in this regard.
Given the prevalence of resistant organisms, it is best to initiate therapy with broader coverage and then narrow therapy in response to the sensitivities of the infecting organism(s).
As S. pneumoniae is the most common, ceftriaxone (or cefotaxime) should be administered. In areas of lower rates of resistance, and meningitis and gram negative bacteria are not suspected, intravenous penicillin may be employed. If a patient has a history of anaphylaxis to penicillins or cephalosporins, vancomycin is a reasonable choice. If H. influenzae or N. meningitidis are suspected, ceftriaxone (or cefotaxime) provide good empiric coverage; aztreonam (or a fluoroquinone with good gram negative coverage such as ciprofloxacin or levofloxacin) can be used in patients severely allergic to penicillin and cephalosporins. Adult dosages may be found in Table 6a and pediatric dosages in Table 6b.
If meningitis is suspected, higher dose ceftriaxone or cefotaxime should be infused along with vancomycin. If there is high level resistance to ceftriaxone (MIC µ2 mg/L), and dexamethasone was given, some would add rifampin along with the vancomycin. A fluoroquinolone with high activity against S. pneumoniae, such as moxifloxacin, has been suggested, but clinical data is not available. Chloramphenicol, if available, may still be useful in the United States in cases of Neisseria meningitidis. Data suggest that aztreonam can be used successfully to treat gram negative meningitis (18).
If the history suggests travel to areas endemic for Babesia, specific therapy will need to be utilized to treat this infection (see below). Capnocytophaga appears sensitive to third generation cephalosporins, but is resistant to aztreonam. Specific recommendations are listed in Table 7a with dosages in Table 7b. In vitro sensitivities against Bordetella holmesii show limited activity of beta-lactams against this agent; carbapenems and fluoroquinolones have low MICs against this agent (30).
Syndromes
Sepsis and DIC (Disseminated intravascular coagulation)
Goal-directed therapy has shown increased survival with reduced morbidity. While beyond the scope of this discussion, the approach to sepsis, specifically severe sepsis and septic shock, is to reverse, as quickly as possible, abnormal hemodynamics and organ dysfunction. Emergent care is provided in the first hour, followed by critical care as discussed below. Antibiotic therapy, as previously described, should be administered and adjusted per culture and sensitivity reports.
Meningitis
Administration of antibiotics should be rapidly accomplished and not delayed for imaging or lumbar puncture. In general, higher dosages (both an increase in the amount of antibiotic and the frequency in which it is administered) are required due to decreased penetration across the blood brain barrier, even if it is compromised by inflammation.
Antibiotic Therapy Directed Against Specific Pathogens (Tables 7a and 7b)
Streptococcus pneumoniae
Penicillins remain the drug of choice for this agent, but increasing rates of resistance and questions regarding the appropriateness of current MIC values have complicated recommendations but clinically have not changed outcomes (20,23,34). For severely ill patients, such as septic shock or meningitis, antibiotic choice is predicated on coverage for the most resistant isolates. In general, penicillin or a third generation cephalosporin will be sufficient without the addition of vancomycin or rifampin which are used as listed in Table 7 for meningitis cases.
Salmonella Species
Antibiotic therapy should be reserved for septicemia and chronic infections such as osteomyelitis, when confirmed. Surgical debridement is frequently required for successful therapeutic outcome. As resistance is not uncommon, sensitivities should be determined to assist in choosing an appropriate antimicrobial.
Capnocytophaga canimorsus
Amoxicillin-clavulanate or ampicillin-sulbactam are the preferred agents for treatment. β-lactamase activity has not been seen in this species, but as related organisms in the genus have acquired this resistance, it would seem prudent to anticipate the possibility. Also, as this organism is usually acquired by trauma from an animal bite, it is a reasonable assumption that other organisms may also be present and they may be producing β-lactamases.
Non-Antibiotic Management
Sepsis and DIC
A patient in respiratory distress should be intubated to maintain oxygenation and ventilation. The circulatory system should be maintained by fluids, vasopressors, inotropes and red blood cell transfusion that the mean arterial pressure is greater than 65 mm Hg, the central venous pressure maintain a range of 8-12 mm Hg, the hematocrit is greater than 30% and the central venous oxygen saturation (ScvO2) above 70%.
Activated protein C (rhAPC), or drotrecogin, should be considered for patients with an APACHE II score of 25 or greater or the failure of 2 or more organ systems. Exclusion criteria require careful consideration (pregnancy, obesity, platelet count less than 30,000 /mm3, aseptic pancreatitis, and others) (1,3). Bleeding appears to be the most significant complication with this agent. Neurological assessments should be made frequently, and if there is change, APC should be stopped and neuro-imaging be obtained. Gastrointestinal bleeding can be detected by testing stool for occult blood, if there is doubt regarding the presence of blood in the stool. The hematocrit and coagulation factors should be monitored.
If, after an assessment of adrenal insufficiency via a stimulation assay, there appears to be adrenal dysfunction, the patient might benefit from therapy with hydrocortisone. Difficulties with variability, reproducibility and interpretation of stimulation assays make providing firm recommendations difficult.
Hyperglycemia occurs frequently and should be managed aggressively, usually with intravenous insulin per established institutional protocol.
Meningitis
In many cases, the care necessitated by severe sepsis or septic shock will be required when meningitis is suspected or has occurred. If shock is not present, dexamethasone 10 mg, four times daily for four days should be administered. If shock is present, low dose steroids may be employed (as per comments above).
Increased intracranial pressure, due to meningoencephalitis, portends a dismal outcome. Cerebral infarcts may also proceed in an ineluctable course. On the other hand, acute hydrocephalus may be successfully managed by repeated lumbar punctures, placement of a drain or a ventriculostomy.
Babesia and Plasmodium
In situations of increasing parasitemia, red blood or whole blood exchange has been used. Whether this modality provides a survival benefit in either Babesia or Plasmodium is unknown and remains controversial (13).
ENDPOINTS FOR MONITORING THERAPY
In general, meningitis due to S. pneumoniae is treated for 7 to 10 days. Pneumonia and septicemia may be adequately treated for 5 to 7 days with oral medication finishing out the course if the patient has deverfesced by day 3 or so. For a patient who is not responding, a more resistant organism may be present or fluid may have loculated creating an empyema. Other deep sources, such as endocarditis, may also bear consideration.
Haemophilus and Neisseria can be treated for 7 days given that normalization of organ systems, white blood count and temperature have occurred. In some cases, there may be persistent end organ damage which should be excluded for purposes of the determination of the duration of antibiotic therapy.
For other organisms discussed, duration of therapy is as previously noted or dictated by the site of infection, i.e., treatment of Salmonella osteomyelitis for four to six weeks.
It would seem reasonable to treat Capnocytophaga for 10-14 days if reasonable improvement were seen. Duration of therapy for Bordetella holmesii is not known, but 10-14 days can be cautiously advised.
Complications and Their Management
For patients requiring ventilatory support for more than two weeks, tracheostomy is usually recommended. Acute respiratory distress syndrome is not an uncommon complication of severe sepsis. In renal failure, hemodialysis or related therapy may be required in the interim or permanently.
If peripheral gangrene has occurred, debridement and, at times, amputation may be necessary.
PREVENTION (Table 8 and Table 9)
Pneumococcal Vaccination
This is the single most important immunization in preventing OPSI. As most cases today are caused by S. pneumoniae (21), it is imperative that patients receive this vaccine. The question of the timing of administration frequently arises. In cases of trauma, as the splenectomy cannot be planned, it is reasonable to vaccinate as soon as possible. However, one study has shown that maximum levels of antibodies form two weeks after splenectomy; waiting four weeks does not improve antibody formation appreciably. For those patients who may be lost to follow-up, I favor vaccination prior to discharge, but lower antibody levels are seen 1 or 7 days after splenectomy compared to 14 days afterwards. Vaccination is clearly better than no vaccination (28,29). For elective splenectomy, vaccination should be provided 14 days before the procedure.
The heptavalent pneumococcal conjugate vaccine (PCV7) is recommended for all children aged 2-23 months with additional doses recommended for children aged 24-59 months with sickle cell disease and other sickle cell hemoglobinopathies, congenital or acquired asplenia or splenic dysfunction. (5,8). It is similar to the Haemophilus influenzae type b conjugate vaccine in involving T cells for its immunogenicity.
Functional or anatomic asplenic adult (aged 19-64) patients (elective and traumatic splenectomy, sickle cell disease) are given the 23-valent pneumococcal polysaccharide vaccination (PPV23). While PCV7 appears to be more immunogenic than PPV23, as the latter provides potentially broader coverage, re-immunization with PCV7 is not recommended. A second dose of PPV23 five years later completes the series. If aged > 65 and vaccinated > 5 years previously when aged <65, one-time revaccination is all that is needed (7).
Other Vaccination
Hib conjugate vaccination has proved very effective in dramatically reducing the incidence of this agent. The clinical experience with Hib is strongest in the pediatric population. It is approved for children aged 6 weeks to 71 months. The final dose of the series is given at > 12 months. Guidelines for administration in adolescents and adults are necessarily vague due to lack of clinical data. If the vaccine is to be administered, the usual dosage is used; currently, there is no recommendation for repeat vaccination. Cases of OPSI due to this agent are extremely rare today.
N. meningitidis vaccine is frequently recommended in asplenia, but is probably not warranted unless living in a region of endemicity. The CDC/ACIP recommends meningococcal polysaccharide vaccine (MPSV4), as a single dose, ages 2-10 if asplenic. Meningococcal conjugate vaccine (MCV4) is recommended for ages 11-55 and greater, again, as a single dose (4). Routinely, MCV4 is recommended for adolescents aged 11-12 (age 15 entering high school) and matriculating freshmen who will be living in dormitories.
Both MPSV4 and MCV4 promote antibody formation against capsular types A, C, Y and W-135. In the United States, type B is the most common. New Zealand has developed a monovalent vaccine against type B which has shown efficacy, but is not without controversy (22). Several reports of Guillain-Barré syndrome have been reported to the Vaccine Adverse Event Reporting System following vaccination with MCV4 (6).
Influenza vaccination is recommended yearly in the asplenic population given the propensity for secondary bacterial sepsis. While in past years there have been problems with limited availability, currently, there are no shortages. The threat of virulent influenza is of great concern and much attention is directed towards it today.
Prophylactic Antibiotics
Although no hard data exist, I believe that most adolescents and adults will not require prophylactic antibiotics. If the risk appears to be relatively high, the patient can be provided with a prescription to keep antibiotics for prophylactic use on hand. For example, a patient who will be traveling and more than an hour away from medical care, should carry a supply of antibiotic with him. If kept cool and dry, it can be expected that potency will be maintained for at least a year. The patient should be instructed to rotate his stock periodically. Amoxicillin-clavulinic acid is a reasonable recommendation (875 mg by mouth twice daily with food for adults, 45 to 90 mg/kg in divided doses twice daily in children). Regardless, if the patient develops a significant fever, especially in the absence of other complaints, he should seek professional care immediately. The patient must be informed that overwhelming and life-threatening sepsis can occur within hours. Severe sepsis and septic shock may occur years after splenectomy.
Other choices for antibiotic prophylaxis include penicillin or amoxicillin, and in penicillin-allergic patients, trimethoprim-sulfamethoxazole or clarithromycin may be substituted.
Until age 5, amoxicillin 20 mg/kg daily or PCN V-K 125 mg twice daily by mouth has displayed clinical utility. One study showed an 84% reduction in sepsis in children aged less than 3 years of age (14). For children over the age of 5 who have undergone splenectomy, twice daily administration of PCN V-K 250 mg for one year after the procedure has been suggested. Some authorities would recommend at least two years while others staunchly support life-long daily antibiotic prophylaxis (33). Even so, break-through infections and sepsis may occur and the patient should be counseled accordingly. Finally, immunizations should be administered on schedule whether or not prophylactic antibiotics are administered.
Tick, Mosquito and Animal Bites
Female mosquitoes feed on mammalian blood. Besides using appropriate antimalarial prophylaxis (chloroquine in limited areas; atovaquone/proguanil, mefloquine, doxycycline in P. falciparum-resistant areas), asplenic patients should be instructed to wear clothing that covers most of their bodies (long sleeves and pants). DEET (30-35%) applied to clothing and, when necessary, non-sensitive, exposed skin. Skin application should be repeated at least every six hours depending on degree of strenuous activity.
Similar advice should be rendered for travel in Babesia-endemic areas. Because the primary vector is the deer tick, Ixodes scapularis, and is quite small (the nymph is 2.5 mm), the patient may not be aware that significant contact has occurred. The patient should receive instructions as discussed in the prevention of mosquito contact. Furthermore, the patient should examine himself carefully for the presence of ticks. As a tick may feed for hours to days, it is possible that earlier detection, albeit difficult, might prevent infection of Babesia or other infective species transmitted by Ixodes (15).
Animal bites should be avoided, especially those involving canids. Children are at increased risk given their smaller size and proportionally greater weakness. If bitten, the wound needs to be cleaned with copious amounts of water, with a gentle skin cleanser and then covered with a clean, dry dressing. Emergent care may be required for deep and/or multiple wounds. Prophylactic antibiotics (for example, amoxicillin-clavulanate or, in the case of penicillin allergy, doxycycline orclindamycin) are prescribed. Tetanus vaccination status needs to be determined and vaccine administered if more than ten years since the previous injection. For adults, if it has been more than two years since the last vaccination, TDaP (Adacel) can be given to provide preventative coverage against Pertussis.
Availability of Medical Information
When emergent medical care is required, the availability of the medical history, current medications, prophylactic antibiotics, vaccination history and contact information may prove life-saving. An asplenic patient should be encouraged to keep this information readily available and on his person as much as is reasonable. There are commercially available identification bracelets, in a variety of designs, which may also be useful. For a fee, some providers can be contacted or accessed directly for the necessary information.
CONCLUSION
While the anatomic or functional asplenic patient is at greatest risk for overwhelming infection immediately after the development of asplenia, the possibility of overwhelming sepsis spans the lifetime of the patient. Certain organisms have a greater incidence and proclivity of infection in this population and preventive measures should be tailored accordingly.
Immunoprophylaxis, chemoprophylaxis, and education are necessary to help prevent OPSI and physicians need to be instructed and willing to use this information in the care of their patients (26,32).
Immunization against these remains the most effective means of preventing morbidity and mortality; the importance cannot be over-emphasized. Antibiotic therapy may be required and should take into account resistance patterns, both locally and nationally, travel history and animal exposure, especially in the presence of trauma associated with animal bites. While several guidelines have been formulated, further research will hopefully clarify areas of ignorance and controversy (17,33).
The patient needs clear and comprehensive instruction about these risks. Measures used to prevent exposure to biting arthropods and reinforcement about the dangers inherent to animal bites must be provided. Antibiotic prophylaxis may be of benefit, in some sub-populations more than others, but requires careful review with the patient to minimize the misuse of antibiotics.
In the presence of significant fever, the patient must seek professional care as rapidly as possible.
REFERENCES
1. Abraham E, Laterre P-F, Garg R, Levy H, Talwar D, Trzaskoma BL, François B, Guy JS, Brückmann M, et al. Drotrecogin alfa (activated) for adults with severe sepsis and a low risk for death. N Engl J Med, 2005; 353 (13): 353: 1332-41.[PubMed]
2. Backhus LM, Bremner RM. Images in Clinical Medicine. Intrathoracic splenosis after remote trauma. N Engl J Med, 2006; 355(17): 1811. [PubMed]
3. Bernard GR, Vincent J-L, Laterre P-F, LaRosa SP, Dhainaut J-F, Lopez-Rodriguez A, Steingrub JS, Garber GE, et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. New Engl J Med, 2001; 344(10): 699-709.[PubMed]
4. Centers for Disease Control and Prevention. Prevention and control of meningococcal disease: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR, 2005; 54(No. RR-7): 1-15. [PubMed]
5. Centers for Disease Control and Prevention. Preventing pneumococcal disease among infants and young children: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR, 2000; 49(No. RR-9): 4-27.
6. Centers for Disease Control and Prevention. Update: Guillain-Barré syndrome among recipients of Menactra® meningococcal conjugate vaccine–United States, June 2005-September 2006. MMWR, 2006; 55 (41): 1120-4. [PubMed]
7. http://www.cdc.gov/Nip/recs/adult-schedule.pdf. Accessed December 20, 2006.
8. http://www.cdc.gov/nip/recs/child-schedule-4pg-landscp.pdf. Accessed December 20, 2006.
9. de Gans J and van de Beek D. Dexamethasone in adults with bacterial meningitis. New Engl J Med, 2002; 347(20): 1549-56. [PubMed]
10. Di Sabatino A, Rosado MM, Ciccocioppo R, Cazzola P, Morera R, Corazza GR, Carsetti R. Depletion of immunoglobulin M memory B cells is associated with splenic hypofunction in inflammatory bowel disease. Am J Gastroenterol, 2005; 100(8): 1788-95.[PubMed]
11. Doll DC, List AF, Yarbro JW. Functional asplenism. South Med J, 1987; 80(8): 999-1006. [PubMed]
12. Ferguson A. Hazards of hyposplenism. Br Med J, 1982. 285: 1375-6. [PubMed]
13. Fraser IP, Cserti CM and Dzik WH. Case records of the Massachusetts General Hospital. Case 32-2006. A 3-year-old girl with fever after a visit to Africa. New Engl J Med, 2006; 355(16): 1715-22. [PubMed]
14. Gaston MH, Verter JI, Woods G, Pegelow C, Kelleher J, Presbury G, Zarkowsky H, Vichinsky E, Iyer R, Lobel JS, et al. Prophylaxis with oral penicillin in children with sickle cell anemia: a randomized trial. N Engl J Med, 1986; 314(25): 1593-9. [PubMed]
15. Goddard J. Physician’s guide to arthropods of medical importance, 4th ed. Boca Raton: CRC Press, 2003; Pp: 399-414.
16. Gutierez F, Masia M, Rodriguez JC, Ayelo A, Soldan B, Cebrian L, Mirete C, Royo G, Hidalgo AM. Evaluation of the immunochromotographic Binax NOW assay for detection of Streptococcus pneumoniae urinary antigen in a prospective study of community-acquired pneumonia in Spain. Clin Infect Dis, 2003; 36(3): 286-92. [PubMed]
17. Howdieshell TR, Heffernan D, Dipiro JT and the Therapeutic Agents Committee of the Surgical Infection Society. Surgical infection society guidelines for vaccination after traumatic injury. Surg Infect (Larchmt), 2006; 7(3): 275-303.[PubMed]
18. Lentnek AL, Williams RR. Aztreonam in the treatment of gram-negative bacterial meningitis. Rev Infect Dis, 1993; 13 Suppl 7: S586-90. [PubMed]
19. Lutwick LI. Infections in asplenic patients. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and practice of Infectious Diseases, 6th ed. Philadelphia: Elsevier Churchill Livingstone, 2005. Pp: 3524-32.
20. Mufson MM, Chan G, Stanek RJ. Penicillin resistance not a factor in outcome from invasive Streptococcus pneumoniae community-acquired pneumonia in adults when appropriate empiric therapy is started. Am J Med Sci 2007; 333(3): 161-7.[PubMed]
21. Norris RP, Vergis EN, Yu VL. Overwhelming postsplenectomy infection: a critical review of etiologic pathogens and management. Infect Med, 1996; 13(9): 779-83.
22. O’Hallahan J. Meningococcal B immunisation programme update. http://www.immunise.moh.govt.nz/documents/menzb-update-oct06.pdf. Accessed December 20, 2006.
23. Peterson LR. Penicillins for treatment of pneumococcal pneumonia: does in vitro resistance really matter? Clin Infect Dis 2006; 42 (2): 224-33. [PubMed]
24. Rushton TC, Gorse GJ, and Bowdler AJ. The relationship of the spleen to infection. In: Bowdler AJ, ed. The complete spleen. Totawa, NJ: Humana Press, 2002; Pp: 175-191.
25. Russell JA. Management of sepsis. New Engl J Med, 2006; 355(16): 1699-1713. [PubMed]
26. Sarangi J, Coleby M, Trivella M, Reilly S. Prevention of post splenectomy sepsis: a population based approach. J Public Health Med, 1997; 19(2): 208-12. [PubMed]
27. Schilling RF. Estimating the risk of sepsis after splenectomy in hereditary spherocytosis. Ann Intern Med, 1995; 122: 187-8. [PubMed]
28. Shatz DV, Romero-Steiner S, Elie CM, Holder PF, Carlone GM. Antibody responses in postsplenectomy trauma patients receiving the 23-valent pneumococcal polysaccharide vaccine at 14 versus 28 days postoperatively. J Trauma, 2002; 53(6): 1037-42. [PubMed]
29. Shatz DV, Schinsky MF, Pais LB, Romero-Steiner S, Kirton OC, Carlone GM. Immune responses of splenectomized trauma patients to the 23-valent pneumococcal polysaccharide vaccine at 1 versus 7 versus 14 days after splenectomy. J Trauma, 1998; 44(5): 760-5. [PubMed]
30. Shepard CW, Daneshvar MI, Kaiser RM, Ashford DA, Lonsway D, Patel JB, Morey RE, et al. Bordetella holmesii bacteremia: a newly recognized clinical entity among asplenic patients. [PubMed]
31. van de Beek D, de Gans J, Tunkel AR, Wijdicks EFM. Community-acquired bacterial meningitis in adults. New Engl J Med, 2006; 354(1): 44-53. [PubMed]
32. Williams DN, Kaur B. Postsplenectomy care: strategies to decrease the risk of infection. Postgrad Med, 1996; 100(1): 195-8. [PubMed]
33. Working party of ASID. Recommendations for the prevention of post-splenectomy sepsis. http://www.racp.edu.au/asid/splenectomy_guidelines0906.pdf. Accessed September 28, 2006.
34. Yu VL, Chiou CC, Feldman C, Ortqvist A, Rello, J, Morris AJ, Baddour LM, et al. An international prospective study of pneumococcal bacteremia: correlation with in vitro resistance, antibiotics administered, and clinical outcome. Clin Infect Dis, 2003; 37(2): 230-7.[PubMed]
Tables
Table 1: Causes of Functional Asplenia
| Congenital | Asplenia Cyanotic heart disease |
| Hematological | Sickle-cell disorders Essential thrombocytopenia Hodgkin’s lymphoma Non-Hodgkin’s lymphoma Fanconi’s syndrome |
| Autoimmune | Systemic lupus erythematosus Mixed connective tissue disease Rheumatoid arthritis Sjögren’s syndrome |
| Gastrointestinal | Celiac disease Ulcerative colitis Crohn’s disease Tropical sprue Whipple’s disease Alcoholic liver disease |
| Circulatory compromise of the spleen | |
| Miscellaneous | Irradiation Amyloidosis Sarcoidosis AIDS Allogeneic Bone Marrow Transplantation Long-term intravenous nutrition Selective IgA deficiency |
Table 2: Pathogens associated with OPSI
| Definite |
Capnocytophaga canis (Dysgonic fermenter 2 [DF2]) Babesia microtis (cattle malaria) Plasmodia spp. (malaria) |
| Possible | Haemophilus influenzae type b (Hib) Salmonella species |
| Unlikely |
Table 3: Differential Diagnosis
Sepsis (infection) with severe sepsis/septic shock |
Painful crisis (sickle cell disease) |
Acute chest pain syndrome (sickle cell disease) |
Pneumonia (without severe sepsis/septic shock) |
Malignancies (lymphoma, leukemia and others) |
Infarction of lung and other cardiopulmonary compromise |
Collagen-vascular disorders |
Drug-associated fever |
Table 4: Clinical Manifestations
Fever with rigors |
Arthralgias and myalgias |
Gastrointestinal symptoms (upper and lower GI tracts) |
Cardiovascular collapse |
Disseminated intravascular coagulopathy |
Seizures |
Coma |
Gangrene (Purpura fulminans) |
Table 5: Laboratory and Radiological Investigations
Routine |
||
|---|---|---|
Complete chemistry profile |
|
|
Complete blood count and differential |
|
|
Coagulation assays |
|
|
Arterial blood gases |
|
|
Peripheral smear |
|
|
Fibrin, fibrin split products |
|
|
Cortisol level |
Cosyntropin stimulation test, if required |
|
At least two sets, two separate sites |
|
|
Urinalysis |
Urine culture, if indicated |
|
Sputum specimen |
Culture and Gram’s stain |
|
Cerebrospinal fluid |
Cell count, protein, glucose |
Gram’s stain, culture |
S. pneumoniae urine antigen |
|
|
Specialized |
||
Buffy coat |
if neutropenic |
|
Plasmodia spp. |
Thin blood smear |
ParaSight F and OptiMal rapid assays |
Thin blood smear |
IgG IFA assay (CDC) |
|
Radiology |
||
Chest radiography |
|
|
Ultrasonography |
As indicated by clinical or laboratory findings |
|
CT and MRI scans |
As indicated by clinical or laboratory findings |
|
Nuclear scans |
As indicated by clinical or laboratory findings |
|
Table 6a: Empiric Antibiotic Therapy, Adults
Antibiotic (trade) |
Usual dosage |
Meningitis dosage |
Renal adjustment |
|---|---|---|---|
Cefotaxime(Claforan) |
1-2 gr IV every 8 hrs |
2 gr IV every 4-6 hrs |
Increase interval to 12-24 hrs |
Ceftriaxone(Rocephin) |
1 gr IV once daily |
2 gr IV every 12 hrs |
Not applicable |
1 gr IV every 12 hrs, Pharmacokinetics recommended |
Same; pharmacokinetics recommended |
Reduction required; antibiotic levels require monitoring |
|
Ciprofloxacin (Cipro) |
400 mg IV every 12 hrs or 500-750 mg PO every 12 hrs |
400 mg IV every 12 hrs or 750 mg PO every 12 hrs |
50% reduction |
Levofloxacin(Levaquin) |
750 mg IV/PO daily |
Same |
750 mg IV/PO once, then 500 mg IV/PO every 48 hrs |
Moxifloxacin(Avelox) |
400 mg IV/PO every 24 hours |
Same |
Clinical data lacking for CNS infections |
Imipenem (Primaxin) |
500 mg IV every 6 hrs |
Same |
125-250 mg IV every 12 hrs; beware of inducing seizures if dosage is exceeded |
Meropenem(Merrem) |
1 gr IV every 8 hrs |
Same |
0.5-1 gr IV every 12-24 hrs |
Table 6b: Empiric Antibiotics Therapy, Pediatric
Antibiotic (trade name) |
Usual dosage |
Meningitis dosage |
|---|---|---|
Cefotaxime (Claforan) |
50 mg/kg IV every 8 hrs |
75 mg/kg IV every 6 hrs |
Ceftriaxone (Rocephin) |
50 mg/kg IV every 24 hrs |
100 mg/kg IV every 24 hrs |
Imipenem (Primaxin) |
15-25 mg/kg every 6 hrs (maximum dosage 2-4 gr/day) |
Not recommended due to seizure potential |
Meropenem (Merrem) |
60-120 mg/kg IV divided every 8 hrs |
120 mg/kg IV divided every 8 hrs |
Rifampin (Rifadin) |
10 mg/kg PO/IV daily |
Same |
40 mg/kg IV divided every 6-8 hrs |
60 mg/kg IV divided every 6-8 hrs |
|
Fluoroquinolones |
not approved for this population, in this setting |
not approved for this population, in this setting |
Table 7a: Organism-Directed Antibiotic Therapy
Organism |
Recommended Antibiotic(s)
|
Alternative(s) |
Comment(s) |
|---|---|---|---|
Penicillin (PCN) MIC<0.1 mg/L |
PCN G or ampicillin |
|
|
PCN MIC 0.1-1.0 mg/L |
cefotaxime or ceftriaxone |
|
|
PCN MIC ≥2.0mg/L |
vancomycin plus ceftriaxone/cefotaxime (plus rifampin if dexamethasone is used) |
Regimen formeningitis; clinical data unavailable for fluoroquinolones |
|
Cefotaxime or ceftriaxone MIC ≥1.0mg/L |
vancomycin plus ceftriaxone/cefotaxime ± rifampin |
moxifloxacin, levofloxacin |
Regimen for meningitis; clinical data unavailable for fluoroquinolones |
H. influenzae (type b and others) |
|||
Beta-lactamase negative |
ampicillin |
cefotaxime, ceftriaxone, cefepime, chloramphenicol, moxifloxacin, levofloxacin, ciprofloxacin |
|
Beta-lactamase positive |
ceftriaxone, cefotaxime |
cefepime, chloramphenicol, moxifloxacin, levofloxacin, ciprofloxacin |
|
PCN MIC <0.1 mg/L |
PCN G or ampicillin |
ceftriaxone, cefotaxime, chloramphenicol |
|
PCN MIC 0.1-1.0 mg/L |
ceftriaxone, cefotaxime |
Chloramphenicol, moxifloxacin, levofloxacin, ciprofloxacin, meropenem |
|
Salmonella species |
Ceftriaxone, cefotaxime, ciprofloxacin, levofloxacin |
Use ampicillin only once sensitivities are known. Meropenem is preferred agent for CNS infections |
|
Imipenem, ertapenem, meropenem,clindamycin, rifampin,doxycycline,erythromycin, vancomycin, cefotaxime, ceftriaxone, ciprofloxacin, levofloxacin |
Resistant to aztreonam. |
||
imipenem, carbapenem, ciprofloxacin, levofloxacin |
|
Beta-lactams are not advised. |
|
Atovaquone plus azithromycin |
Clindamycin plus oralquinine |
For dosages, see table 7b. |
|
Plasmodia spp. |
|
|
|
Severe, non-pregnant |
quinidine gluconate plus doxycycline or clindamycin |
and primaquine (for non-falciparum spp.) |
For dosages, see table 7b. |
Pregnant, not severe |
quinine sulfate plus clindamycin |
Quinine sulfate plus doxycycline (if preferred regimen failing) |
primaquine, if necessary, after delivery to treat non-falciparum; avoid mefloquine; for dosages, see table 7b. |
Table 8: Recommended Vaccines
Vaccine |
Adult |
Pediatric |
Booster |
Comment |
|---|---|---|---|---|
|
|
|
|
|
Pneumococcal conjugate vaccine (PCV-7) (Prevnar) |
See PPV |
Age ≤23 months: 4 doses at 2, 4, 6 and 12-15 months (0.5 ml IM thigh or deltoid) |
PPV-23 at age ≥ 2 y/o Give ≥2 mos after last PCV; 0.5 ml IM/SC; repeat 3-5 yrs later |
PCV not for use in children >59 months old |
Pneumococcal polysaccharide vaccine (PPV-23) (Pneumovax) |
0.5 ml IM/SC |
See PCV |
Repeat ≥5 yrs If age ≥65 and ≥5 yrs since last dose |
Only two doses in lifetime are recommended |
|
||||
|
|
|
Hib/DTaP (TriHIBit) and Hib/HepB (COMVAX) are also available |
|
PRP-OMP (PedvaxHIB) |
0.5 ml IM |
Two doses two months apart beginning at 2 months old (0.5 ml IM) |
Age 12-15 months (may use TriHIBit also) (0.5 ml IM) |
No clinical data for adults, but appears well tolerated; only one dose is recommended |
HbOC (HibTITER), PRP-T (ActHIB), |
0.5 ml IM |
6 weeks to 71 months: Three doses two months apart beginning at 2 months old (0.5 ml IM) |
Age 12-15 months (may use TriHIBit also) (0.5 ml IM) |
No clinical data for adults, but appears well tolerated; only one dose is recommended |
|
||||
|
|
|
CDC continues to recommend; please see comments in text. |
|
Quadravalent polysaccharide vaccine (MPS4) (Meromune) |
0.5 ml SC |
Age ≥ 2 years; 0.5 ml SC |
Provides protection for 3-5 yrs ; revaccinate for high risk situations |
Covers A,C, Y and W-135 |
Quadrivalent conjugate vaccine (MCV4) (Menactra)
|
Ages 11-55 ; 0.5 ml IM deltoid |
Age ≥ 1 ; 0.5 ml IM deltoid |
Unknown |
Covers A,C, Y and W-135 |
Monovalent MC type B |
|
|
|
Not available in United States |
|
||||
|
|
|
|
|
Injectable (Fluvirin, Fluzone, Fluarix) |
0.5 ml IM deltoid |
Ages 6 months-8 yrs: 2 injections at least 4 weeks apart for first time recipients; ages 6-35 months: 0.25 ml IM, ant-lat thigh Ages 3-8 yrs: 0.5 ml IM ant-lat thigh or deltoid (older children) |
Yearly |
Fluvirin approved for ≥5 yrs; Fluarix approved for ≥18; optimally administer October- November |
Intranasal (LAIV) (Flumist) |
Age ≥ 12 years but ≤ 49 years: 0.5 ml intranasal |
Ages 5-8: two doses 0.5 ml intranasal 6-10 weeks apart; if first dose was injectable, wait 4 weeks. Ages ≥9 years: 0.5 ml intranasal |
Yearly |
Avoid in pts severely immuno- compromised or in those who will be exposed to severely immuno- compromised |
Table 9: Prevention
Immunization: S. pneumoniae, Influenza virus, Hib; possibly N. meningitidis |
Tick, mosquito and animal bite prevention |
Oral antibiotic prophylaxis |
Availability of medical and contact information, i.e, medical bracelet |
Early intervention with appropriate support and antibiotics |
Guided Medline Search For:
Norris RP, et al. Overwhelming Postsplenectomy Infection: A Critical Review of Etiologic Pathogens and Management. Infect Med 1996;13:779-783.