
Fever in Patients with Cancer
Authors: Mark A. Marinella, MD, FACP, FACN, CNSP
EPIDEMIOLOGY AND PATHOPHYSIOLOGY
Malignancy and Fever
It is well-known that cancer, diagnosed or undiagnosed, can cause fever. Indeed, fever from underlying malignancy accounts for up to 25% of cases of fever of underdetermined origin in some series. Furthermore, lymphoma is the most common etiology of neoplastic fever of underdetermined origin. The pathophysiology of tumor-induced fever may be due to several mechanisms (Table 1) of which include release of cytokines from tumor cells or infiltrating mononuclear cells (e.g., tumor necrosis factor and interleukin-1); necrosis of tumoral tissue; or obstruction of a hollow duct or viscus resulting in proximal infection (e.g., a cholangiocarcinoma causing biliary obstruction and ensuing suppurative cholangitis). Other causes of fever in the cancer patient include drug fever (e.g., antibiotics, chemotherapy drugs); thrombotic thrombocytopenic purpura (TTP; which may result from chemotherapy or the tumor itself); and deep venous thrombosis/Trousseau’s syndrome.
Specific Cancers That Induce Fever
Cancer fever classically is associated with Hodgkin’s lymphoma, but can occur in the setting of non-Hodgkin’s lymphoma, leukemia, and solid tumors (Table 2). Some specific solid malignancies that result in tumor fever include renal cell carcinoma (by elaboration of interleukin-6), hepatocellular carcinoma, pancreatic carcinoma, bronchogenic carcinoma, and brain tumors. A unique benign tumor which may present with fever is atrial myxoma, a tumor notorious for releasing cytokines which cause constitutional symptoms. A good rule of thumb, however, is to consider cancer of any type in a patient with prolonged fever and no evidence of infectious illness.
Fever Patterns
In most patients, no particular fever pattern emerges that is pathognomic of cancer. Fever can occur during the day or night, although drenching night sweats are often a manifestation of malignancy and, if persistent, should prompt the clinician to consider neoplastic disease. Physicians should counsel their patients with suspected persistent fever to keep a temperature diary, taking their temperature at periods throughout the day and night in order to assess any underlying pyrexial pattern.
A sudden-onset fever with rigors and chills is concerning for bacteremia, which may complicate viscus obstruction as noted above, or febrile neutropenia. A fever without concomitant rise in pulse (“temperature-pulse dissociation, or Faget’s sign) may signify drug fever, use of beta-blocker drugs, or infection with intracellular organisms. Afternoon fever is purported to be suggestive of intrabdominal abscess. Pel-Epstein fever is the prototype fever associated with Hodgkin’s lymphoma and consists of several days of fever separated by afebrile episodes of similar duration, typically 7 to 14 days. However, this is an uncommon fever pattern, and its absence should in no way dissuade the clinician from the diagnosis.

Chemotherapy-Induced Fever
A useful clinical dictum is that not all fever in the cancer patient (or any patient for that matter) is due to an infectious process. Although the wise clinician always searches for life-threatening infection at the outset, consideration of other causes may be warranted if no infection is isolated. Chemotherapeutic and biologic drugs that have been implicated in causing fever include azathioprine, hydroxyurea, interleukin-2, rituximab, and interferon. Fever is attributed to numerous chemotherapy drugs as an uncommon or rare occurrence. The clinician should check drug compendiums or with their hospital pharmacy if any particular drug is suspect in causing fever.
Exposure Risk Factors
Exposure to certain drugs or microbes may induce fever in the cancer patient. For a discussion of neutropenic fever please refer to that specific chapter in this book. As far as certain exposures causing fever in patients with cancer, a useful approach involves considering the patient with an undiagnosed (or suspected) malignancy or the patient with an established diagnosis of cancer.
The Patient with Undiagnosed (or Suspected) Cancer
Patients with previously undiagnosed, but suspected, cancer may develop fever from exposure to infectious agents, especially if they have myeloma or leukemia. For instance, patients with chronic lymphocytic leukemia may be hypogammaglobulinemic and be prone to infection with encapsulated bacteria such as Streptococcus pneumoniae. Also, a patient with undiagnosed advanced Hodgkin’s lymphoma with splenic involvement may be functionally asplenic and prone to sepsis when exposed to a dog bite (Capnocytophagia canimorsus sepsis), to people with meningococcal disease, or to Vibrio vulnificus infection if exposed to raw shellfish.
The Patient with Known Cancer
Patients with cancer are exposed to a variety of treatment situations, blood products, and medications that may induce fever. For instance, a patient with a prolonged hospitalization and immobility may develop a blood clot in their leg, leading to fever. Also, the cancer patient may be exposed to nosocomial bacteria, which can cause infection and fever. Transfusion of blood products can induce fever via immune mechanisms, antigens, or even bacterial contamination (especially with platelet transfusions). As a final example, drug exposures can lead to fever, as discussed above. A notable example relevant to the oncologic patient is thrombotic microangiopathy that can complicate mitomycin-C or gemcitabine administration.
DIFFERENTIAL DIAGNOSIS
Infection
Bacterial Versus Viral Infection
The astute, thoughtful clinician always entertains infection as a possible cause of fever in any patient, especially those with cancer since these patients are especially prone to infection. Bacterial infections of the respiratory and urinary tracts predominate. However, other sites include the sinuses, mouth, abdomen, skin and soft tissue, and bloodstream. The most common microbes isolated from the blood include Gram-positive cocci (e.g., Staphylococci and Streptococci) and Gram-negative bacilli, such as theEnterobacteriaciae and Pseudomonas species. Pneumococcal pneumonia and E. coli urinary infections remain common in cancer patients as well. Table 3 displays some of the common infection types in cancer patients and Table 4 displays some of the more frequently isolated bacterial species.
An in-depth discussion of microbiology is beyond the scope of this text, but viral pathogens may infect patients with solid tumors and hematologic malignancies, especially leukemics who have had total marrow ablation for a bone marrow transplant. Some of the viruses that may cause infection in these groups include Cytomegalovirus, Epstein-Barr virus, Adenovirus, Echovirus, Influenza A virus, respiratory syncytial virus, Parvovirus, and human herpes virus-8. If any of these pathogens are suspected, an infectious diseases consultation should be considered since viral infections are often difficult to diagnose, and often even harder to treat.
Risk Factors for Infection
Venous Catheters
Indwelling central venous catheters for long-term chemotherapy or parenteral nutrition place the cancer patient at significant risk for bloodstream infection, especially with Staphylococcal species. Implanted surgical ports, central venous lines, or peripherally inserted central catheters (PICC) lines may all become infected, especially if strict aseptic technique is breached during insertion or port manipulation. A central catheter can become infected in three primary ways. First, during insertion, bacteria on the skin can infect the insertion tract, thereby contaminating the soft tissue which can lead to a tunnel or soft tissue infection. The bacteria can migrate along the line into the bloodstream resulting in bacteremia. A second way a central line can become infected is thru contamination of the port during drug or fluid administration. Third, the line itself can become colonized after insertion and lead to bacteremia. Some pathogens (e.g., Staphylococcus sp. Pseudomonas sp. and Candida sp.) produce a biofilm on the catheter which prevents immune cells from destroying the bacteria as well as decreasing antibiotic efficacy. As a result, one should consider line removal if catheter-associated bloodstream infection is diagnosed.
Chemotherapy Induced Mucositis
The intent of systemic chemotherapy is to arrest growth and destroy actively dividing neoplastic cells. However, rapidly proliferating cells of the oral and alimentary mucosa are also susceptible to chemotherapy resulting in cell death, inflammation, and regeneration. This denudation of the oral and gut mucosa (“mucositis”) may lead to bacterial translocation with fever and sepsis, especially with Gram-negative bacilli and microaerophilic streptococci.
Surgical Procedures
Surgery results in disruption of normal tissue and organs and invokes a reparative and inflammatory response. Cancer surgery (e.g., breast, colon, other viscera) often results in large incisions and, at times, empty tissue spaces that can fill with fluid or blood and become infected. Cancer patients with immune dysfunction, neutropenia, or recent chemoradiotherapy administration are more prone to developing wound and incision infections or, less commonly, a bacterial infection at the surgical bed site, resulting in fever. Fever in patients who have had cancer surgery may also result from venous thrombosis, drug fever, or catheter-related infection. Also, it is prudent to remember that surgery itself results in liberation of cytokines from migrating leukocytes at the interface of surgery-induced tissue trauma, which can also cause fever.
Foreign Bodies
Cancer patients with implanted foreign bodies may develop fever as an immune reaction to the device or due to subsequent infection. For instance, a cancer patient with a neoplastic fracture of the femoral neck may require a palliative hip hemiarthroplasty. Fever is almost universal following prosthetic joint implantation and is due to mononuclear cells releasing cytokines that cause fever. As noted, foreign body infection can also cause fever. Cancer patients may have pre-existing prosthetic heart valves that could become seeded with bacteria during chemotherapy-induced mucositis. Prosthetic joints, pacemaker wires, surgical drains, ventriculo-peritoneal shunts, and surgical mesh to repair an abdominal wall defect following cancer surgery are other examples of foreign bodies that can become infected leading to fever.
Miscellaneous
Other risk factors for infection in this population include bedrest with subsequent decubiti formation or aspiration pneumonitis; long-term broad spectrum antibiotics for neutropenic fever resulting in candidemia; mucormycosis of the nasal cavity complicating metabolic acidosis or hyperglycemia; and necrotizing fasciitis or Fournier’s gangrene in patients with breeches of the skin.
Non-Infectious Etiologies
Deep Venous Thrombosis
Venous thromboembolism (VTE) is an important diagnosis that may cause fever in the cancer patient and should be considered in any patient without clear evidence of infection-associated fever. Many tumor histologies have been linked to venous thrombosis, but adenocarcinomas of the breast, lung, prostate, alimentary tract, and kidney are most common. These tumors create a biochemical hypercoagulable state by secreting various clotting factors. Classically, migratory thrombophlebitis, known as Trousseau’s syndrome, is a harbinger of cancer, usually visceral (especially pancreatic). Brain tumors, lymphoma, and melanoma may also be associated with venous thromboembolism.
Other reasons that cancer patients are predisposed to venous thromboembolism include immobility, surgery, venous occlusion or stasis from tumor masses or lymphadenopathy, dehydration, and endothelial injury from chemotherapy. As a result, the clinician needs to maintain a high index of suspicion of venous thromboembolism in any febrile cancer patient, and realize that venous thromboembolism may coexist with ongoing infection.
A unique manifestation of hypercoagulability, especially with adenocarcinomas, is non-bacterial thrombotic endocarditis (NBTE), or marantic endocarditis. This phenomenon results in sterile vegetations that typically occur on the mitral or aortic valves. Fever may be a prominent manifestation, as well as peripheral vascular or central nervous system embolic phenomena, which can be devastating.
Tumor Fever
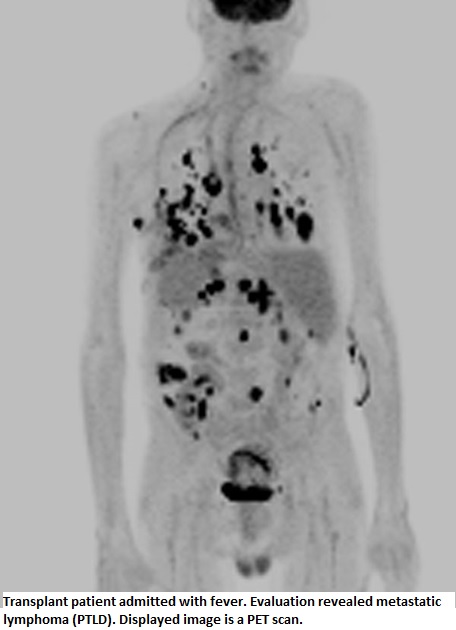
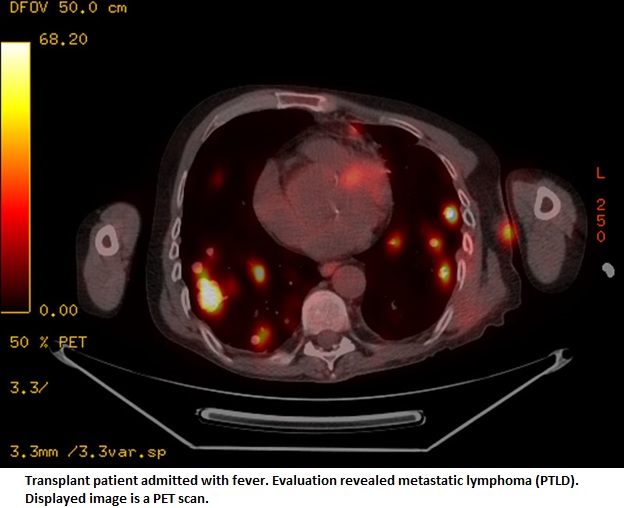
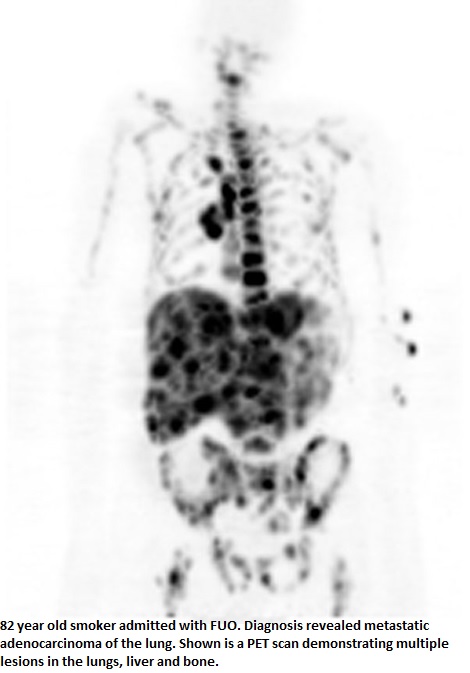
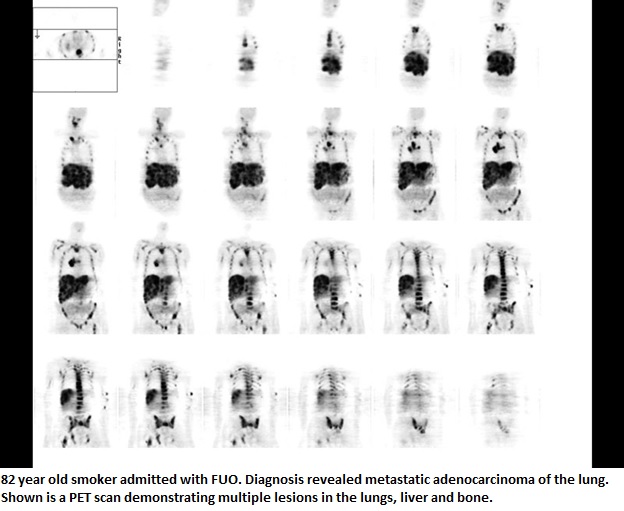
As noted above, various neoplasms can invoke a febrile response by liberating cytokines such as interleukin-2, TNF, interleukin-6, amongst others. Some of the tumors classically associated with tumor-induced fever include renal cell carcinoma, atrial myxoma, non-Hodgkin’s lymphoma ![]() , Hodgkin’s lymphoma, and leukemia. Many other solid tumors
, Hodgkin’s lymphoma, and leukemia. Many other solid tumors ![]() have been implicated in causing tumor fever as well, but an in-depth discussion of this topic is beyond the scope of this text.
have been implicated in causing tumor fever as well, but an in-depth discussion of this topic is beyond the scope of this text.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Drug Fever
Various classes of drugs can invoke a febrile response. One of the challenges of evaluating fever in a cancer patient is the protean differential diagnostic possibilities of fever in this population such as infection, neoplastic tissue, thrombosis and various drugs. Chemotherapeutic agents, antibiotics, and other drug classes can cause fever, which often make pinning down the etiology very difficult. Suffice it to say, the clinician should consider drug fever as a possible cause of fever in the cancer patient, especially in the presence of rash, eosinophilia, or temperature-pulse dissociation. Table 5 lists some of the more notable causes of non-infectious fever in the cancer patient.
DIAGNOSIS OF FEVER IN THE PATIENT WITH CANCER OR SUSPECTED CANCER
Clinical Clues
History
As in all areas of medicine, the history is the crux of diagnosis in the febrile patient. Many historical clues may elicit the cause of fever, but only a few will be noted since not all scenarios can be covered in this limited space. Drenching night sweats, significant weight loss, and anorexia often accompany fever complicating neoplastic disease, especially Hodgkin’s or non-Hodgkin’s lymphoma. Fullness or a “dragging” sensation in the left upper quadrant may signify splenic enlargement that may complicate chronic myelogenous leukemia or disseminated lymphoma. Rigors and chills during the daytime should make the physician consider infection, although some tumors can evoke chills as well. Fever and early satiety may indicate gastric cancer or extrinsic impingement upon the stomach wall by intra-abdominal lymphadeonpathy or splenomegaly from lymphoma. Fever and hemoptysis may be due to lung cancer or post-obstructive pneumonia resulting from a thoracic mass lesion such as bronchogenic carcinoma or massive lymphadenopathy from lymphoma. Alternatively, immunosuppressed cancer patients could develop reactivation tuberculosis or a fungal infection which may cause fever, systemic symptoms, and hemoptysis. To summarize, a thorough history in any febrile patient is the cornerstone to a prompt, accurate diagnosis.
Physical Examination
In febrile patients with known cancer or those undergoing chemotherapy, the physical examination should focus on potential sites of infection such as the oral cavity, nasal sinuses, neck, chest, abdomen, perineum, perirectal area, skin, and joints. Febrile patients with undiagnosed but suspected cancer should also have a thorough search for infection. In addition, major lymph node chains should be thoroughly palpated (e.g. neck, supraclavicular, occipital, axillae, epitrocholear, inguinal, popliteal areas) since enlargement of lymph nodes in these areas may occur with lymphomas, leukemias, and metastatic adenocarcinoma. The presence of a supraclavicular node (Virchow node) should prompt a search for intrathoracic or visceral malignancy. A peculiar lymph node lesion known as the Sister Mary Joseph nodule is invariably associated with metastatic intra-abdominal cancer (e.g., ovary, gastric, etc.). Another area to focus attention on in a febrile patient with suspected cancer includes the skin, since metastatic renal cell or bronchogenic cancer may involve the integument as may leukemia (“leukemia cutis”). A palpable renal mass may signify renal cell carcinoma, which can cause fever, systemic symptoms, hematuria, and multiple laboratory derangements earning this neoplasm the title of the “Internist’s tumor.” A unique cause of fever and systemic illness in a leukemic patient receiving chemotherapy is typhlitis, an inflammatory/infectious phlegmanous process involving the appendix and cecum. Physical examination may reveal right lower quadrant tenderness, rebound tenderness, or a doughy, mass-like area to palpation.
Fever Curves
No fever pattern is specific for any type of malignant disease. As noted in a preceding section, the Pel-Ebstein fever pattern is classically associated with Hodgkin’s lymphoma. This pattern manifests as episodic fever at various times of day and in various intervals, typically consisting of a three to ten day period of fever, followed by a three to ten day period of apyrexia. Nonetheless, it is best to remember that any prolonged fever can be associated with a variety of solid and hematologic cancers.
Non-steroidal Anti-inflammatory (NSAID) Challenge
Diagnosing cancer rests on collection and analysis of multiple data sets of which include history, physical examination, laboratory and serologic studies, radiography, and tissue biopsy. However, at times the diagnosis of prolonged fever can remain elusive despite the initial evaluation. Chang and colleagues demonstrated that the NSAID agent naproxen was very effective in suppressing tumor fever and this property may be useful in elucidating the clinician’s suspicion of cancer in patients with prolonged, undiagnosed fever. Naproxen has been the classically touted agent for suppressing tumor fever due to its unique ability to suppress tumoral cytokines in preference over infectious cytokines. While the “naproxen challenge” may be useful in evaluating prolonged fever suspected to be of neoplastic origin, it must be utilized in the context of a thorough, clinically-driven assessment.
LABORATORY ASSESSMENT
Infectious Disease Evaluation
Other chapters in this work cover this aspect in greater detail, but a few salient features of an infectious work-up in the febrile cancer patient will be mentioned.
Cultures
Cultures of the blood, urine, and sputum are fairly standard in any cancer patient suspected of having a bacterial infection. Cultures of other body fluids should be based on the clinical situation but include cerebrospinal fluid, pleural fluid, peritoneal fluid, or abscess fluid. Typically, culture of these sites requires an invasive procedure.
Patients suspected of having a bacterial infection due to a fastidious bacterial organism (e.g., nutritionally deficient streptococci) or a virus require special media and notification of the microbiology laboratory. In this circumstance, Infectious Disease consultation should be arranged.
Serologies/Antigen Studies
Acute and convalescent serologies for viral infections may be useful, as may heterophile tests for cytomegalovirus or Epstein-Barr virus. If Legionella infection is suspected, the urine antigen study is approximately 70% sensitive for detecting infections with Legionella pneumophilia, serogroup 1. For more discussion on serologic and antigenic testing, the reader is referred to specific chapters in the Microbes section. Acute Phase reactants Supplemental testing in the diagnosis of fever in the cancer patient may include many laboratory tests, most of which are non-specific.
Acute Phase Reactants
The ESR is a non-specific test of systemic inflammation which measures the distance a drop of blood falls within a microtube in one hour. The result is reported in mm/hr, and values of greater than 100 mm/hr are suggestive of malignancy, deep seated infection, or autoimmune disease. However, the ESR is only a general screen as to the presence of systemic inflammation and is by no means diagnostic of any disease process. C-reactive protein is an acute phase reactant produced by hepatocytes, and may be elevated in the same clinical scenarios as the ESR. Again, this test is not diagnostic of cancer and shares the limitations of the ESR, but may be more sensitive to diagnose an inflammatory process.
Radiology
When to Order Computed Tomographic (CT) Scanning
CT scanning has revolutionized the diagnostic approach to a variety of diseases, especially cancer. Fever in the cancer patient can be due to neoplasia itself which can manifest on CT imaging as a primary mass lesion, metastases, body cavity effusions, pneumonia, hydronephrosis, biliary dilatation, and lymphadenopathy. Perhaps the greatest utility of CT imaging is the ability to obtain a tissue diagnosis with aspiration cytology or a needle core biopsy. As such, CT imaging should be considered in a febrile patient when cancer is suspected, when a tissue diagnosis is needed, or if an infectious process may be present.
When to Order Magnetic Resonance Imaging (MRI)
Fever in a patient with known or suspected cancer can typically be diagnosed with history, physical examination, basic laboratory studies, and CT scanning. The use of MRI is more limited in this situation but may prove helpful for diagnosing pancreatico-biliary neoplasms (with magnetic resonance cholangiopancreaticography, MRCP), soft tissue or muscle tumors, or even bone sarcomas or osteomyelitis. Occasionally, brain metastatisis or gliomas can induce fever, and cerebral MRI is very sensitive in diagnosing brain lesions.
When to Order Nuclear Medicine Imaging
Nuclear imaging studies are occasionally helpful in evaluating fever in the cancer patient. Technitium bone scanning is useful in assessing for osseous metastases, especially osteoblastic metastases. Indium-111 scanning may assist in the diagnosis of an abscess or infected fluid collection. Gallium-67 scanning has been utilized in the diagnosis of lymphoma. Perhaps the most useful nuclear imaging test is positron emission tomography (PET) scanning which utilizes radio-labeled glucose (typically 18-flourodeoxyglucose, FDG) to identify areas of increased metabolic activity that occur with a variety of neoplasms, such as lung cancer and lymphoma. Not only is PET making an impact in diagnosis of malignancy but also on the assessment of recurrence after surgery or chemotherapy. This modality may also identify areas of focal inflammation or infection, which can make diagnosis challenging in certain patients.
EMPIRIC ANTIBIOTIC THERAPY
Empiric Antibiotics Versus Watchful Waiting
Other chapters in this text address antibiotic therapy in the cancer patient in more detail. However, a few basic principles will be discussed. First and foremost, any cancer patient with febrile neutropenia (absolute neutrophil count <500 cells/mm3) should be rapidly assessed to identify an obvious infectious source. In general, any patient with neutropenia and fever with unstable vital signs, acidosis, clouded sensorium, or co-morbidities should be admitted and administered broad-spectrum anti-microbials (e.g., ceftazidime, piperacillin-tazobactam). Febrile neutropenic patients who are clinically stable and appear well can be managed as an outpatient with oral agents such as a fluoroquinolone combined with amoxicillin-clavulonate. For a more detailed discussion, the reader is referred to other chapters in this text or to textbooks in medical oncology.
ADJUNCTIVE THERAPY
Supportive Care
General medical care should be offered to the cancer patient with fever and typically includes intravenous fluids to replace insensible water loss from pyrexia, pain control, venous thromboembolism prophylaxis, nutrition support, and physical therapy. This should all be done simultaneously with fever evaluation.
Antipyretic Therapy
Fever is a normal host response to inflammation and infection and may confer an immunologic benefit, especially in patients with bacterial infection. Nonetheless, anti-pyretic therapy with acetaminophen, aspirin, or NSAIDS may be considered in certain situations. First, if a patient requests fever suppression for comfort, it should be provided. Another indication for treatment of fever is the potential adverse effects of fever-induced insensible water loss and increased metabolic demands in ill patients with multiple co-morbidities, especially the elderly. In addition, sinus tachycardia from fever can lead to decreased filling of the ventricle and result in congestive heart failure in patients with limited cardiac reserve. In general, acetaminophen is the agent with the most favorable side-effect profile since it lacks gastropathic and nephrotoxic effects at clinical doses, although caution should be exercised in patients with significant liver disease.
Naproxen Challenge Test
In 1982, Chang and Gross published the sentinel paper on the use of naproxen in the diagnosis of cancer-induced fever. They noted that 14 of 15 patients found to have a malignant disease had suppression of fever when naproxen 375 mg was administered orally twice daily for three days. This was in distinction to the group of eight patients with documented infection of whom only one patient experienced lysis of their fever. Other authors have noted similar results with naproxen, and although not pathognomic for cancer fever, the naproxen challenge test may be useful in narrowing down the cause of undiagnosed fever when cancer is suspected.
READING LIST
Brusch JL, Weinstein L. Fever of unknown origin. Med Clin North Am 1988;72:1247-61. [PubMed]
Chang JC, Gross HM. Utility of naproxen in the differential diagnosis of fever of undetermined origin in patients with cancer. Am J Med 1984:76:597-603. [PubMed]
Cunha BA. Fever in malignant disorders. Infect Dis Pract 2004;29:335-6. [PubMed]
Cunha BA. Fever of unknown origin. Infect Dis Clin North Am 1996;10:111-27. [PubMed]
Marinella MA. Oncologic Disorders. In: Recognizing Clinical Patterns: Clues to a Timely Diagnosis. Philadelphia: Hanley and Belfus, 2002, pp. 123-145.
Marinella MA. Thrombotic thrombocytopenic purpura. In: Frequently Overlooked Diagnoses in Acute Care. Philadelphia: Hanley and Belfus, 2003, pp. 107-110.
Petersdorf RG, Beeson PB. Fever of unexplained origin: report on 100 cases. Medicine (Baltimore) 1961:40:1-30.
Scanlon GT, Castellino RA, Rudders R. Lymphographic demonstration of cyclic changes in lymph node size during Pel-Epstein fever. Cancer 1975;36:2026-2028.[PubMed]
Tables
Table 1: Mechanisms of Fever in Cancer Patients
Cytokine release by tumor
|
| Tumor necrosis/inflammation |
Tumor obstruction of tubular or hollow structure and subsequent infection
|
| Venous thrombosis/thrombophlebitis |
| Hypothalamic metastases (altered thermoregulation) |
Medications
|
Table 2: Neoplasms That Commonly Cause Fever
|
Table 3: Infections That May Affect Cancer Patients
|
Table 4: Bacteria That Cause Infection in Cancer Patients
| Gram positive organisms |
|---|
| Staphylococcus aureus |
| Staphylococcus epidermidis |
| Streptococcal species (S. pyogenes, agalactiae, pneumoniae; Group C, G) |
| Enterococcal species (E. faecalis, faecium) |
| Gram-negative organisms |
| Eschericia coli |
| Pseudomonas spp. |
| Haemophilus influenzae |
| Proteus spp. |
| Enterobacter spp. |
| Citrobacter spp. |
| Stenotrophomonas spp. |
| Legionella spp. |
Table 5: Non-Infectious Etiologies of Fever in the Cancer Patient
| Venous thromboembolism/Trousseau’s syndrome |
| Non-thrombotic (“marantic”) endocarditis |
| Disseminated intravascular coagulation (DIC) |
Thrombotic microangiopathy
|
| Transfusion reactions |
| Neoplasms (see Table 2) |
| Foreign bodies (e.g., artificial joints, drains, stents) |
| Surgical procedures |
| Mucositis |
| Hematoma |
Medications
|
Torres JP, et al. Frequency and Clinical Outcome of Respiratory Viral Infections and Mixed Viral-bacterial Infections in Children with Cancer, Fever and Neutropenia. Pediatrc Infect Dis J 2012;31:889-893.