
Headache
Authors: Roland Jones, M.D., Bradley Jacobs, M.D., M.S.
Headache is commonly defined as head pain (cephalgia) not limited to the distribution of a cranial or cervical nerve (neuralgia).
The International Headache Society (IHS) criteria for headache classification divides headache into primary and secondary disorders (5). Primary headaches such as migraines and tension type headaches are the most common headaches, and have a benign nature. Primary headache disorders are diagnosed by clinical history and physical examination using the diagnostic criteria as set forth in the International Classification of Headache Disorders (ICHD) (5). Primary headache disorders, by definition and by diagnostic criteria, cannot be attributed to another disorder. Secondary headache disorders result when another underlying organic disorder leads to cephalgia. Secondary headaches may require additional tests beyond history and physical examination to confirm or exclude certain etiologies. Secondary headaches may be associated with significant morbidity and therefore warrant more urgent evaluation and perhaps even empiric treatment.
Epidemiology
Headaches are a common problem, impacting both quality of life and occupation. It has been reported that 15% of adults have been absent from work in the past twelve months due to headache (13). The one-year prevalence of headache varies widely from 51-91% (3, 13). Two percent of all patients presenting to the emergency room have headache as their chief complaint (9). In studies of the general population, the lifetime prevalence for any type of headache ranges from 69 to 99% (Table 1 and Table 2). Tension headache is more prevalent than migraine. Both migraine and tension type headache are more common in women. Many have established histories of chronic primary headache disorder and present with recurrent headache. Underlying central nervous system disease is relat ively uncommon in the population of patients suffering from headache. However, up to one-third of patients presenting to emergency rooms with a chief complaint of abrupt onset headache, may have potentially fatal or disabling intracranial pathology (4). In the case of giant cell arteritis (temporal arteritis), the incidence increases with age, peaking in the range over seventy years old. It is rarely seen in people younger than 50. Approximately 45% of the cases are associated with polymyalgia rheumatica (15).

Pathogenesis
Modern neuroscience has seen much progress in the explanation of the pathogenesis of headaches in the past two decades, but much is still unknown. Primary headache pathogenesis is complex involving sterile neurogenic inflammation with resultant plasma extravasation (11). Dysregulation of pain mediating neuropeptides such as calcitonin gene-related peptide (CGRP) is a contributing factor (11). Ultimately, the caudal trigeminal nucleus is the neuronal structure responsible for nociceptive information of the cranial structures. Neuronal activity may be dysregulated within this nucleus as well as with its relationship with higher order pathways involving the midbrain in patients with primary headache disorders (11).
The pathogenesis of secondary headache relates to nociceptive receptors being activated by an underlying pathology. Brain parenchyma itself is not capable of relaying nociceptive information, rather it relies on intracranial pain sensitive structures such as the dura matter, cervical and cranial arteries and veins, the ear, the eye and orbits, and portions of the cranial and cervical nerves.
Differential Diagnosis
The differential diagnosis of cephalgia includes primary headache syndromes such as migraine, cluster, and tension headaches, and numerous heterogeneous disorders including infections causing secondary headaches. With secondary headaches (Table 3 and 4), cephalgia may be experienced when the intracranial pain sensitive structures are affected by various processes such as intracranial neoplasm, infections, arterial thrombosis or dissection, hemorrhage, cerebral edema and elevated intracranial pressure, inflammation, metabolic derangement, toxic exposure and others (4, 7, 9).
Clinical Manifestations
Clinical history and physical examination are the most important element in headache diagnosis. Clinicians should be searching for symptoms and signs (Table 6) that raise concern for potentially disabling secondary causes of headache (AKA “red flags”) (1, 3, 7, 9). These patients may require prompt laboratory or radiographic investigation, empiric therapy, or both. Abrupt onset of headache suggests a secondary cause and thus a higher potential for being disabling if not rapidly diagnosed and treated (4). Additionally, patients with known systemic disease or immunocompromised state are more likely to have secondary headaches and underlying causes should be carefully evaluated. Information of headache in theHIV positive patient can be found in the HIV Manual.
The clinician should ask about features of the headache including frequency, severity, location, quality of pain, associated aura and autonomic symptoms. Environmental, dietary, and activity triggers should be identified. Caffeine use and pain medication use or overuse (rebound headache) should be reviewed.
A patient with a primary headache disorder will typically have a reassuring history of similar previous headaches or family members with a similar headache history. In patients with recurring headaches, features most suggestive of migraine include nausea, phonophobia, photophobia, exacerbation by physical activity, and an aura (Table 5) (12). Cluster headaches typically have a distinct clinical pattern of unilateral symptoms lasting 45 minutes to 3 hours peaking within 10 to 15 minutes to an excruciating periorbital quality. Some patients report even considering suicide during these attacks due to the severity. Autonomic symptoms such as rhinorrhea and lacrimation are noted by up to 80% of these patients. Attacks occur daily for a period of consecutive days (11), often at the same time of day. Tension headaches are recurrent non-pulsatile bilateral headaches of mild to moderate severity that are not aggravated with routine physical activity (5).
Malignant external otitis can present with severe, often intractable headache. The pain is often nocturnal, awakening the patient from sleep. Earache and temporomandibular joint pain may accompany the headache, and these are clues for this rare infection. Purulent otorrhea is usually present at some point in the past medical history and the patient is classically an elderly diabetic.
Before the use of antibiotics, acute mastoiditis ![]() was the most common complication of acute otitis media (AOM). Antibiotic treatment of AOM has decreased the incidence of acute mastoiditis. Signs of classic mastoiditis include: postauricular fluctuance, bulging erythematous tympanic membrane, erythema and tenderness over the mastoid area, and protrusion of the auricle. Signs of latent mastoiditis include: no external signs of mastoid inflammation, infected or normal-appearing tympanic membrane, recurrent fever. The neurologic examination is typically nonfocal, though, cranial nerve involvement is possible with advanced disease.
was the most common complication of acute otitis media (AOM). Antibiotic treatment of AOM has decreased the incidence of acute mastoiditis. Signs of classic mastoiditis include: postauricular fluctuance, bulging erythematous tympanic membrane, erythema and tenderness over the mastoid area, and protrusion of the auricle. Signs of latent mastoiditis include: no external signs of mastoid inflammation, infected or normal-appearing tympanic membrane, recurrent fever. The neurologic examination is typically nonfocal, though, cranial nerve involvement is possible with advanced disease.
Skull-based osteomyelitis can present insidiously with headache of prolonged duration ![]() that can become excruciating. It can occur from extension of infection from the paransasal sinuses or external auditory canal (malignant external otitis). Rarely, it is a complication of retrograde septic thrombophlebitis. Facial nerve and other cranial nerve palsies can occur with extension of the infection.
that can become excruciating. It can occur from extension of infection from the paransasal sinuses or external auditory canal (malignant external otitis). Rarely, it is a complication of retrograde septic thrombophlebitis. Facial nerve and other cranial nerve palsies can occur with extension of the infection.
Sinusitis is a common cause of headaches. Acute bacterial rhinosinusitis (ABRS) is a secondary bacterial infection of the nose and paranasal sinuses, usually preceded by a prolonged viral upper respiratory tract infection. Viral and bacterial rhinosinusitis are difficult to differentiate. These infections cause an inflammatory response involving the mucosa of the nose and paranasal sinuses, which results in symptoms such as nasal obstruction, purulence, postnasal drip, facial pressure and pain, alteration in the sense of smell, cough, fever, halitosis, fatigue, dental pain, and ear pressure and fullness.
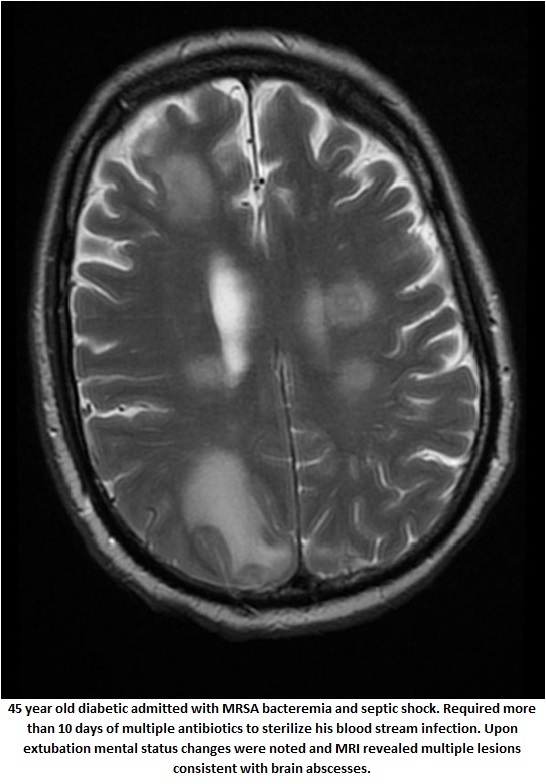
A brain abscess ![]() presents clinically in a nonspecific manner, often resulting in a delayed diagnosis (mean 13-14 days after onset of symptoms). Headache is the most common symptom, usually localized to the side of the abscess, and its onset can be gradual or sudden. Fever is not always present (10). The pain tends to be severe and not relieved pain medications. Mental status changes are indicative of cerebral edema while vomiting is associated with increased intracranial pressure (2). Fifteen percent of patients will have neck stiffness, especially when purulence has leaked into a lateral ventricle.
presents clinically in a nonspecific manner, often resulting in a delayed diagnosis (mean 13-14 days after onset of symptoms). Headache is the most common symptom, usually localized to the side of the abscess, and its onset can be gradual or sudden. Fever is not always present (10). The pain tends to be severe and not relieved pain medications. Mental status changes are indicative of cerebral edema while vomiting is associated with increased intracranial pressure (2). Fifteen percent of patients will have neck stiffness, especially when purulence has leaked into a lateral ventricle.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagnosis
Diagnosis of headache relies on the clinician’s history and physical examination. Neuroimaging, lumbar puncture, serology and other studies will be directed by these clinical clues.
All patients with “red flags” by history or physical exam (Table 6) should undergo prompt neuroimaging. Neuroimaging can be pivotal in the diagonsis of subarachnoid hemorrhage, brain tumor or abscess, malignant external otitis, skull-based osteomyelitis and sinusitis. Cranial CT is faster and more readily available and is therefore done prior to cranial MRI. Patients with suspected trauma related headaches should undergo urgent CT imaging of the head. CT without contrast is sufficient to rule out hemorrhage but if tumor or abscess is suspected and MRI is not easily available (or the patient has a contraindication to MRI), CT with contrast should be considered. When the CT does not reveal abnormalities and diagnosis is still uncertain, MRI with and without contrast should be considered.
If subarachnoid hemorrhage is suspected and CT scan did not reveal hemorrhage, a lumbar puncture should be performed to analyze cell count and xanthochromia (yellowish tinge of CSF that may be related to bilirubin from breakdown of red blood cells). When performing lumbar puncture it is useful to check the cell counts in the first and fourth tubes in order to ease assessment of traumatic lumbar puncture. Appearance of CSF is extremely important (Table 7). If it is clear, this suggests no bleeding. If it is xanthochromic, this suggests subarachnoid hemorrhage. If it is bloody, it is very helpful to spin it down. If the supernatant is clear this suggests, the blood was traumatic. However, if it is xanthochromic, it suggests subarachnoid hemorrhage. In patients with suspected aneurysm or arterial dissection, angiography should be considered.
Patients with signs of meningitis, encephalitis, significantly immunocompromised states, and those with CSF shunts should undergo lumbar puncture for CSF analysis and pressure measurement. Standard CSF testing should include cell counts (in 1st and 4th tubes), glucose, protein, and gram stain and culture (Table 7). Other tests that may be considered depending on the clinical situation include cryptococcal antigen, India ink stain, HSV PCR, VDRL, stain and culture for AFB, fungal culture, and cytology. Remaining CSF fluid after initial testing should be preserved for potential expansion of laboratory evaluation.
In a patient over fifty with a new headache associated with fever, visual complaints, or jaw claudication, a diagnostic evaluation for giant cell arteritis (temporal arteritis or GCA) should be initiated. The erythrocyte sedimentation rate (ESR) has a good negative predictive value. It is elevated to greater than 50 in 96% of cases (15) while elevation of C-reactive protein may aid in diagnosis of those with unimpressive ESR’s. A definitive diagnosis is made by temporal artery biopsy. The temporal artery is often segmentally affected; therefore the biopsy must be of adequate size, usually at least 2 cm. It is unnecessary to delay treatment with prednisone while awaiting the performance or results of a biopsy as the diagnostic findings on biopsy are often present as long as two weeks after initiating corticosteroids (14).
In patients with malignant external otitis, the ESR is virtually always elevated (unless the patient has received partial antibiotic therapy, often with a quinolone), often approaching 100 mm. CT scan may show bony erosion in the temporal bone or mastoid and soft tissue swelling. Definitive diagnosis rests on isolating Pseudomonas aeruginosa from bone. Patients with skull based osteomyelitis are diagnosed based on CT and MRI findings.
Diagnosis of bacterial sinusitis may be made if viral URI symptoms persist for 10 or more days or worsen after 5 to 7 days and are accompanied by the previously mentioned signs and symptoms. Physical exam generally provides only limited information. Imaging studies, such as plain film radiographs, CT scans ![]() , and magnetic resonance imaging (MRI) may be helpful in the management of rhinosinusitis, but because they cannot differentiate between viral and bacterial causes of rhinosinusitis, they are not generally recommended for routine management. CT scan is indicated in complicated cases.
, and magnetic resonance imaging (MRI) may be helpful in the management of rhinosinusitis, but because they cannot differentiate between viral and bacterial causes of rhinosinusitis, they are not generally recommended for routine management. CT scan is indicated in complicated cases.
{kind=link}
{kind=link}
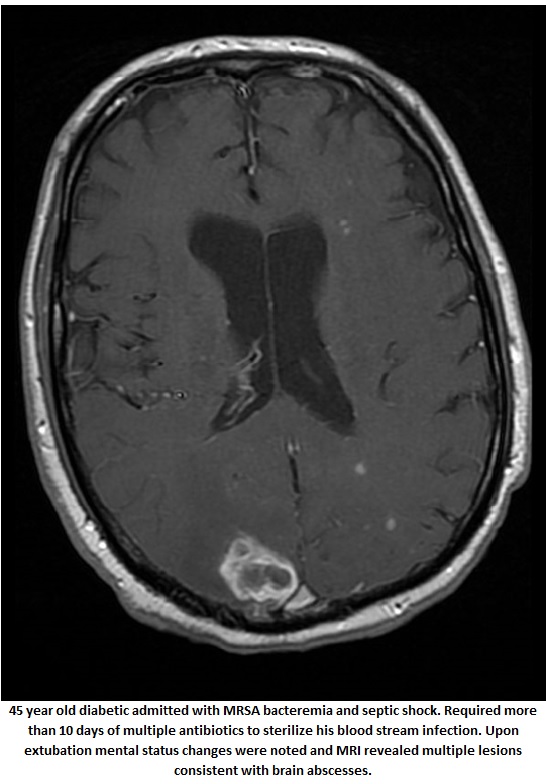
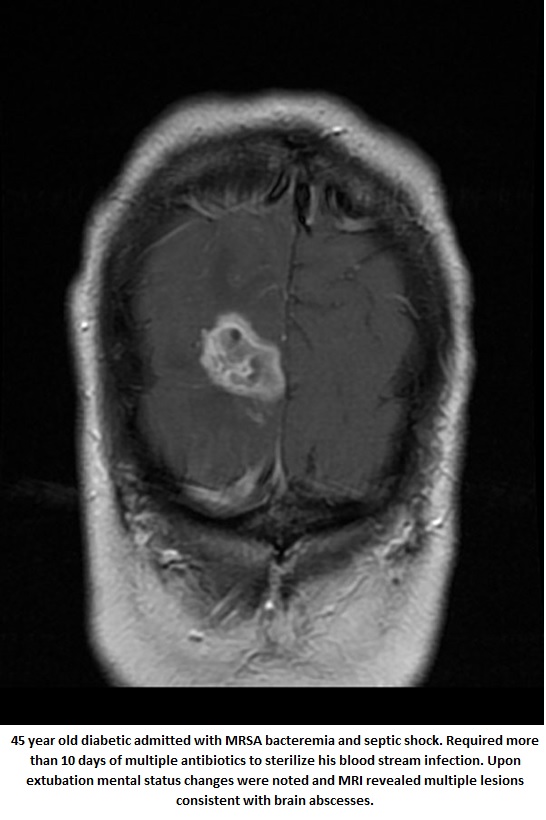
Brain abscesses are diagnosed via imaging studies. CT scan is not as sensitive as MRI for the diagnosis of brain abscess ![]() but can frequently be obtained more easily on an emergent basis (8). If a brain abscess is in the differential diagnosis and MRI cannot be performed, then CT scan with contrast is the diagnostic test of choice. In the setting of focal signs, symptoms or papilledema, a lumbar puncture is contraindicated (6). CT scan with contrast or MRI should be performed prior to lumbar puncture in this situation to exclude a focal cerebral lesion. Blood cultures should be obtained as well.
but can frequently be obtained more easily on an emergent basis (8). If a brain abscess is in the differential diagnosis and MRI cannot be performed, then CT scan with contrast is the diagnostic test of choice. In the setting of focal signs, symptoms or papilledema, a lumbar puncture is contraindicated (6). CT scan with contrast or MRI should be performed prior to lumbar puncture in this situation to exclude a focal cerebral lesion. Blood cultures should be obtained as well.
TREATMENT
Treatment of headaches is based on the type (primary or secondary) and severity of the patient’s headache. A patient’s previous success or failure with a given agents is considered as well as drug side effects and the patient’s comorbidities.
The pharmacologic treatment of migraine is divided into acute (abortive, symptomatic) treatment (Table 8) and preventive (prophylactic) treatment (Table 9). The acute oral treatment of migraine headache is typically accomplished with NSAIDS, triptans, narcotics, antiemetics and occasionally steroids. Intravenous treatment of the acute migraine may involve dihydroergotamine (DHE), narcotics, antiemetics, fluids, anticonvulsants (such as valproate), steroids, and antipsychotics such as chlorpromazine (Thorazine).
Cluster headache poses a unique treatment obstacle because of its short duration. Many of the abortive agents used to treat cluster headache do not reach effective serum concentrations until after the headache has begun to spontaneously resolve. Accordingly, fast acting abortive agents such as oxygen, IM sumatriptan, IV narcotics and fluid in the inpatient setting, and appropriate prophylactic therapy with agents such as calcium channel blockers and lithium are important in the treatment of cluster headaches. Short-term steroids may also be helpful to alleviate an attack.
Secondary headaches are usually managed with NSAIDS and narcotics while the underlying cause is addressed with appropriate therapy. In the case of temporal arteritis, early diagnosis and treatment are essential to prevent blindness. If a patient has symptoms and findings consistent with temporal arteritis, immediate therapy with prednisone 60mg per day should be initiated. Again, it is unnecessary to delay treatment awaiting biopsy results.
Patients with headaches and meningeal signs or meningitis by preliminary CSF studies should be treated empirically with appropriate antibiotics until acute bacterial meningitis has been excluded or cultures and studies allow more specific therapy (Table 10 and Meningitis chapter). Antibiotics should not be delayed while awaiting lumbar puncture, but lumbar puncture should be done within two hours of first antibiotic dose to avoid interference with cultures. The results of CSF analysis should direct further treatment and investigations. Headaches in these patients often respond to NSAIDS and narcotics. Migraine may be triggered by the meningitis and should not be overlooked as migraine specific treatments in these patients may be more useful. Empiric treatments for other infectious causes of headaches are listed in Table 11.
CONCLUSION
Headache is commonly encountered clinical problem. Evaluation should be guided by a detailed patient history and physical examinations. Patients who clinical scenario suggests a secondary cause of headache should undergo appropriate imaging studies and potentially a lumbar puncture. Treatment is based on the type and severity of the headache, a patient’s previous success (or failure) with a given agent as well as drug side effects and the patient’s comorbidities.
REFERENCES
1. Bartleson JD. When and how to investigate the patient with a headache. Semin Neurol 2006;26(2):163-170. [PubMed]
2. Chun CH, Johnson JD, Hofstetter M, Raff MJ. Brain abscess. A study of 45 consecutive cases. Medicine (Baltimore) 1986; 65(6):415-31. [PubMed]
3. Clinch CR. Evaluation of acute headaches in adults. Am Fam Physician 2001;63(4):685-692. [PubMed]
4. Davenport R. Acute headache in the emergency department. J Neurol Neurosurg Psychiatry 2002;72(II):ii33-ii37.[PubMed]
5. Headache Classification Committee of International Headache Society. The International Classification of Headache Disorders. Cephalgia 2004;24:1.
6. Heilpern KL, Lorber B. Focal intracranial infections. Infect Dis Clin North Am 1996;10(4):879-98. [PubMed]
7. Joubert, J. Diagnosisng Headache. Aust Fam Physician 2005;34(8): 621-625. [PubMed]
8. Leuthardt EC, Wippold FJ 2nd, Oswood MC, Rich KM. Diffusion-weighted MR imaging in the preoperative assessment of brain abscesses. Surg Neurol 2002;58(6):395-402. [PubMed]
9. Levin M. The acute severe headache – assessment and treatment. Comp Ther 2002;28(4):235-243. [PubMed]
10. Seydoux C, Francioli P. Bacterial brain abscesses: Factors influencing mortality and sequelae. Clin Infect Dis 1992;15(3):394-401.[PubMed]
11. Silberstein, Lipton, Dalessio. Wolfe’s Headache and Other Head Pain. Oxford Press, Seventh Ed.
12. Smetana G. The diagnostic value of historical features in primary headache syndromes. Arch Intern Med. 2000;160:2729-2737. [PubMed]
13. Stovner LJ, Zwart JA, Hagen K, et al. Epidemiology of headache in Europe. European J Neurol 2006;13:333-345.[PubMed]
14. Tierney L. Current Diagnosis and Treatment. McGraw-Hill, 2003.
15. Widico C. Evidence-based emergency medicine/rational clinical examination abstract. Does this patient have temporal arteritis? Ann Emerg Med 2005;45(1):85-87.[PubMed]
Tables
Table 1. Lifetime Prevalence of Migraine and Tension-Type Headaches in the General Population, by Gender.
|
|
Headache Type |
|
|---|---|---|---|
Country of Study |
Any: M (%) F (%) |
Tension-type M (%) F (%) |
Migraine M (%) F (%) |
Denmark (n=1,000) |
93 99 |
69 88 |
8 25 |
United States (n=1,809) |
83 84 |
42 34 |
41 50 |
United Kingdom (n=727) |
69 94 |
29 35 |
10 26 |
Compiled from HIV Clinical Manual
Table 2. Prevalence of Selected CNS Diseases in People with Headache.
Country of Study |
Vascular Disease (%) |
Tumor (%) |
CNS Infection (%) |
Head Trauma (%) |
|---|---|---|---|---|
Denmark (n=1,000) |
0.5 |
1 |
- |
4 |
United States (n=872) |
0.9 |
- |
0.6 |
9.3 |
Compiled from HIV Clinical Manual
Table 3. Causes of Secondary Headache Syndromes
| Trauma |
|---|
|
| Infection |
|
| Vascular |
|
| Metabolic |
|
| Toxic |
|
| Medications |
See Table 4 |
| Neoplastic |
|
| Other intracranial diseases |
|
| Other non-neurological disease |
|
Table 4. Medications Frequently Associated with Headache.
HIV Medications |
Medications Causing Acute Headache |
Medications Causing Rebound Headache |
Other Substances |
|---|---|---|---|
Indomethacin Nifedipine Cimetidine Atenolol Captopril Piroxicam Metronidazole |
Ergotamines Aspirin Nonsteroidal anti-inflammatory drugs Narcotic analgesics Caffeine |
Heroin Cocaine Marijuana Alcohol Gamma-hydroxybutyrate (GHB) |
Compiled from HIV Clinical Manual
Table 5: ICHD-2 Diagnostic Criteria for Migraine with and without Aura
Migraine with Aura |
Migraine without Aura |
|---|---|
A. At least 2 attacks that fulfill criteria B-D B. At least one of the following, but no motor weakness
C. At least two of the following
D. Headache fulfilling criteria B-D for Migraine without aura begins during theaura or follows aura within 1 hour E. not attributable to another disorder |
A. At least 5 attacks that fulfill criteria B - D B. Headache attacks that last 4 to 72 hours (untreated or unsuccessfully treated) C. Headache has at least 2 of the following characteristics:
D. During headache, at least 1 of the following symptoms:
E. No evidence of related organic disease |
From The International Headache Society
Table 6. Headache History and Examination “RED FLAGS”
“Red Flags” in history
|
Disease
|
|---|---|
“First or Worst” headache |
Subarachnoid hemorrhage or a secondary headache even in an individual with previous primary headache |
New onset headache in a patient over the age of 50 |
Less likely a primary headache syndrome, which typically has onset before age 40 |
Headache worsened by Valsalva |
Mass lesion, elevated intracranial pressure, sub arachnoid hemorrhage |
Abrupt onset |
Subarachnoid or intraparenchymal hemorrhage |
Recent head or neck injury |
Arterial dissection, subdural or epidural hematoma |
New headache that is persistent |
Tumor, CNS infection, vasculitis, elevated intracranial pressure |
Headache that is progressive in quality |
Tumor |
Headache worsened by sitting or standing up |
Low CSF pressure such as in post LP or spontaneous CSF leak |
Systemic features (fever, weight loss) |
Vasculitis, CNS or systemic infection, and sepsis |
Visual disturbances |
Optic neuritis, acute glaucoma, benign intracranial hypertension |
Unilateral persistent headache in an adult , jaw claudication or transient monocular blindness |
Temporal Arteritis |
Associated neck stiffness and fever |
Meningitis and other infections |
|
|
“Red Flags” in Physical Exam
|
Disease |
Elevated Blood pressure |
Hypertensive encephalopathy |
Fever |
CNS infection |
Altered level of consciousness |
Tumor, intraparenchymal hemorrhage or SAH, intracranial hypertension/hydrocephalus, CNS infection |
Hemotympanum, otorrhea, rhinorrhea, mastoid ecchymosis (Battle Sign), Periorbital ecchymosis (raccoon eyes) |
Head Trauma |
Nuchal rigidity, Kernig’s or Brudzinski’s sign |
Meningitis |
Presence of focal neurological deficits |
Tumor, cerebral ischemia, abscess, subdural or epidural hematoma, subarachnoid or intraparenchymal hemorrhage |
Papilledema or retinal hemorrhage |
Elevated intracranial pressure from tumor, optic neuritis, hypertensive encephalopathy, benign intracranial hypertension. |
Headache with rash |
Meningococcal meningitis, lyme disease |
Acute headache in a pregnancy or postpartum |
Cerebral vein/dural sinus thrombosis |
Sinus tenderness, fever, purulent nasal discharge |
|
Table 7. Interpretation of Cerebrospinal Fluid Findings in Patients with Headache
Diagnosis |
Cells/µl |
Glucose (mg/dl) |
Protein (mg/dl) |
Opening Pressure |
|---|---|---|---|---|
Normal |
0-5 lymphocytes |
45-85 (~70% blood glucose level) |
14-45 |
70-180mm H20 |
Bacterialmeningitis |
200-2000 PMN |
<45 |
>50 typically >100 |
Very elevated |
Granulomatous meningitis (mycobacterial and fungal) |
100-1000 WBCs with lymphocytic predominance |
<45 |
>50 typically >100 |
Moderately elevated |
Spirochetal meningitis |
100-1000 WBCs with lymphocytic predominant |
Normal |
>50
|
Normal to slightly elevated |
Viral meningitis/ encephalitis (aseptic) |
25-2000 WBCs with lymphocytic predominant |
Normal or moderately low |
>50 typically >100 |
Slightly elevated |
Abscess (brain and epidural) & Parameningeal Reaction (mastoiditis, sinusitis, septic thrombus) |
Normal to moderately increased WBCs |
normal |
Normal to moderately high (>50) |
Variable |
Subarachnoid hemorrhage |
Early: usually >100,000 RBC; Late: increased WBC |
Normal or decreased |
Early: 50-400 Late: 100-800 |
Increased |
Traumatic (bloody) Tap |
RBC:WBC ratio similar to that in peripheral blood |
Normal |
Slightly increased |
Normal |
Benign intracranial hypertension (Pseudotumor cerebri) |
Normal |
Normal |
Normal |
Increased (>18-20 cm) |
Table 8. Abortive Migraine Therapeutic Options for Adult Patients
Agent |
Action & Comments |
Preparations & Dosing |
|---|---|---|
Ergot Alkaloids |
Vasomotor active and reduces neurogenic inflammation. Can be given IV for severe headaches in an inpatient setting, but patients should be monitored on cardiac telemetry due to coronary vasoconstrictor concerns |
Dihydroergotamine intravenous (DHE) 0.5-1mg IV TID. Dihydroergotamine intranasal (Migranal) |
Morphine and Narcotics |
Potent analgesic effect, but rebound concerns, and does not address migraine pathology |
Morphine Oxycodone/Acetaminophen (Percocet) Hydrocodone/Acetaminophen (Vicodin) |
NSAIDS |
Often used in combination with other agents such as “triple therapy” (NSAID+ Ergot or Triptan + antiemetic) |
Naproxen 500mg PO BID. Ibuprophen 400-800mg PO TID. Toradol 60 mg IM. |
5-HT Agonists (“Triptans”) |
May cause rebound More useful in early migraine and prodrome Reverse neurogenic inflammation. Should not be used in combination with ergots |
Sumatriptan (Imitrex) 25-100mg po, or 6mg SC. Many other “triptan” alternatives |
Steroids |
Useful in pregnancy when many drugs are contraindicated |
Hydrocortisone, Dexamethasone, Methylprednisolone Solu-Medrol 500mg IV BID. |
Valproic Acid |
Oral preparations are used in prophylaxis, but intravenous preparations for abortive therapy |
Intravenous valproic acid (Depacon) 300-1000mg in 100cc NS IV TID given over 30 minutes. |
Phenothiazines & Metoclopramide |
Dopamine antagonist in the chemoreceptor trigger zone as well as peripheral stomach receptors. Intravenous prochlorperazine or chlorpromazine can be used to abortively for severe migraine but are typically given in an inpatient setting due to concerns of hypotensive and extrapyramidal side effects |
Prochlorperazine (Compazine) Promethazine (Phenergan) 12.5-25mg IV TID. Chlorpromazine (Thorazine) 12.5 -25mg IV TID. Metoclopramide (Reglan) 10mg PO |
Table 9. Preventive Medications for Headache.
Drug |
Usual Dosage |
Dose Interval |
Maximum Daily Dosage |
Adverse Effects |
|---|---|---|---|---|
Tricyclic antidepressants (TCA) Amitriptyline
Nortriptyline |
10mg initial, then 100-300mg 10mg initial; then 100-150mg |
qHS
qHS |
300 mg
150 mg |
Sedation especially amitriptyline; dry mouth |
Beta-adrenergic Blockers Propranolol |
40-320 mg |
q12h |
640 mg |
Contraindicated in asthma or congestive heart failure patients. |
Anticonvulsants Valproic acid
|
250-1000 mg
|
q12h
|
2000 mg
|
Confusion, alopecia, weight gain, tremor. Hepatotoxic. |
Gabapentin |
600-1200 mg |
Q8h |
3600 mg |
Somnolence, dizziness, ataxia, and weight gain |
Carbamazepine |
200 mg initially, then 300-1000 mg |
Q12h |
2000 mg |
Nausea, drowsiness, dizziness, ataxia, blood dyscrasias |
Table 10. Empiric Therapy for Suspected Bacterial Meningitis
Predisposing Factor |
Common Bacterial Pathogens |
Antimicrobial Therapy |
|---|---|---|
Age |
||
<1 month |
Streptococcus agalactiae,Escherichia coli, Listeria monocytogenes, Klebsiellaspp. |
Ampicillin + cefotaxime; or ampicillin + an aminoglycoside |
1-23 months |
Streptococcus pneumoniae,Neisseria meningitidis,Streptococcus agalactiae,Haemophilus influenzae, Escherichia coli |
Vancomycin + a third-generation cephalosporina,b |
2-50 years |
Neisseria meningitidis, Streptococcus pneumoniae |
Vancomycin + a third-generation cephalosporina,b |
>50 years |
Streptococcus pneumoniae, Neisseria meningitidis, Listeria monocytogenes,aerobic gram-negative bacilli |
Vancomycin + ampicillin + a third-generation cephalosporina,b |
Head trauma |
||
Basilar skull fracture |
Streptococcus pneumoniae, Haemophilus influenzae, group A β–hemolytic streptococci |
Vancomycin + a third-generation cephalosporina |
Penetrating trauma |
Staphylococcus aureus, coagulase-negative staphylococci (especiallyStaphylococcus epidermidis), aerobic gram-negative bacilli (including Pseudomonas aeruginosa) |
Vancomycin + cefepime; or vancomycin +ceftazidime; or vancomycin + meropenem |
Post-neurosurgery |
Aerobic gram-negative bacilli (including Pseudomonas aeruginosa), Staphylococcus aureus, coagulase-negative staphylococci (especiallyStaphylococcus epidermidis)
|
Vancomycin + cefepime; or vancomycin + ceftazidime; or vancomycin + meropenem |
Cerebrospinal fluid shunt |
Coagulase-negative staphylococci (especiallyStaphylococcus epidermidis),Staphylococcus aureus, aerobic gram-negative bacilli (includingPseudomonas aeruginosa),Propionibacterium acnes |
Vancomycin + cefepimec; or vancomycin + ceftazidimec; or vancomycin + meropenemc |
aCeftriaxone or cefotaxime.
bSome experts would add rifampin if dexamethasone is also given.cIn infants and children, vancomycin alone is reasonable unless Gram’s stain reveals the presence of gram negative bacilli.
From Meningitis Chapter in Empiric
Table 11: Empiric Antibiotic Recommendations for Infectious Causes of Headaches
Condition |
Empiric Antibiotic Recommendations |
|---|---|
Brain Abscess |
Ceftriaxone 2 grams IV q12 hours + metronidazole500 mg IV every 6 hours (Add vancomycin if post-traumatic or post-neurosurgical or if concerned about MRSA ) |
Encephalitis |
Acyclovir 10 mg/kg IV every 8 hours while HSV PCR is pending |
Malignant Otitis Externa
|
Cefepime 2 grams IV every 12 hours or piperacillin4 grams IV every 4 hours or cipro 400 mg IV every 12 hours. May add tobramycin to above if severe infection. Oral outpatient therapy should include cipro 750 mg every 12 hours. |
Acute Mastoiditis |
Ceftriaxone 2 grams IV daily orAmpicillin/sulbactam 2 grams IV every 6 hours. Oral antibiotic options includeamoxicillin/clavulanate 875 mg bid. |
Ceftriaxone 2 grams IV every 12 hours plus vancomycin 15 mg/kg IV every 12 hours. Add ampicillin if concern regarding Listeria. |
|
If antibiotics indicated (duration > 10 days or worsening after 5 days of symptoms and have purulent drainage and significant pain) augmentin 875 po bid, moxifloxacin 400 mg daily orlevofloxacin 500 mg daily. |
|
Skull based osteomyelitis |
Treatment varies by location and comorbidities. |
Guided Medline Search For:
Waldman SD, et al. Headache pain of ear, nose, throat and sinus origin. Med Clin North Am 2013;97:309-319.