
Epstein-Barr Virus Infections
Authors: Sankar Swaminathan, M.D.
Previous Authors: Ming Han Tsai, Li Min Huang, Oriol Manuel, Atul Humar
Epstein-Barr virus (EBV; Human herpesvirus-4) is a human gammaherpesvirus that establishes lifelong infection in B lymphocytes with a predilection for latent, rather than lytic, infection. EBV replicates during lytic infection by mechanisms common to all herpesviruses, and EBV lytic infection is inhibited by nucleoside analogues such as acyclovir, ganciclovir, and foscarnet. However, diseases induced by EBV are frequently associated with latent infection, and nucleoside analogues active against lytic replication may not be effective clinically. Currently, treatment of EBV-associated diseases is more often directed against virus-induced tumors or disease symptoms and less frequently against viral replication. Pharmacologic intervention in pathways important for latent infection, vaccines and other immunologic therapies to prevent infection or attenuate disease are potential areas for therapeutic development.
VIROLOGY
Epstein-Barr virus is a double-stranded DNA virus (82). Human and primate B lymphocytes and to a lesser degree, epithelial cells can be infected in vitro with EBV. After adsorption to the cell surface receptor and virion entry, several Epstein-Barr nuclear antigens (EBNAs) and latent membrane proteins are expressed (1). In vivo, EBV infects lymphocytes resident in tonsillar and oropharyngeal tissue. Whether EBV also infects and replicates in epithelium during primary infection is unknown but no evidence of such replication at the time of diagnosis of symptomatic disease has been found. Infected B lymphocytes become immortalized and proliferate indefinitely in culture. The molecular mechanisms by which EBV latent infection gene products immortalize B cell growth have been characterized over the past two decades. In general these involve viral proteins usurping normal cell signaling pathways involved in cell growth, such as the tumor necrosis factor receptor and Notch ligand receptor pathways. EBV latent proteins also have complex effects on host cell transcription and gene expression. Determining how latent EBV genes function to affect cell growth continues to be an active area of investigation and may provide novel opportunities for pharmacologic intervention in EBV latent infection and associated malignancies. In vitro, only a small fraction of infected cells reactivates lytic infection to produce infectious virions. In latently EBV-infected cells, the virus exists as a circular DNA molecule, or episome, in the nucleus, and viral DNA is replicated in unison with cell DNA and cell doubling.
EPIDEMIOLOGY
Infection with EBV is ubiquitous, with 90-95% of all adults displaying serological evidence of past infection (48). In the United States, approximately 50% of children are seropositive by age five, with a second period of seroconversion occurring in early adulthood (110). Infection occurs earlier in developing countries and in certain areas of the United States. Most cases of EBV infection are transmitted by the presence of virus in oropharyngeal secretions of asymptomatic shedders. Blood transfusions and transplantation of solid organs or bone marrow may also be associated with EBV transmission. While detection of EBV in genital secretions of both men and women has been reported (61, 135), it is unclear whether this is a significant mode of transmission (see below).
Infectious Mononucleosis
Infectious mononucleosis, the syndrome characterized by a classic triad of fever, sore throat and lymphadenopathy (28) (see Clinical Manifestations below) is most commonly caused by primary EBV infection. Infectious mononucleosis is most frequently diagnosed in industrialized countries in young adults. When infection is delayed beyond childhood, the incidence of symptomatic infectious mononucleosis has been estimated to be between 25-75% (100, 129). The higher incidence in this demographic group most likely reflects a later age of primary infection as well as greater access to health care and availability of specific diagnostic tests. Although racial differences in the incidence of infectious mononucleosis have been noted, these are likely to be related to differences in the age at which primary infection occurs (47). The differences observed between infants and young adults with regard to primary infection may relate to the size of the viral inoculum at the time of infection or to the intensity of cellular immune responses driven by EBV-infected B cells. Genetic polymorphisms in the interleukin-10 gene have been linked to severe symptomatic EBV infection (46). Crawford DH, et al. also found a significant association of type 1 EBV with infectious mononucleosis, suggesting that viral determinants may also influence the host response that results in symptomatic infection (22). In a large study of students entering college in the United Kingdom, EBV infection was significantly more common among women than men. A history of sexual intercourse was also significantly associated with prior infection as well as with symptomatic infectious mononucleosis (23). Whether this association merely reflects the presence of other risk factors associated with sexual activity is unknown. EBV is found in the saliva for extended periods after recovery from infection, and has been detected at high titers for median period of 32 weeks after primary infection (9), suggesting that healthy convalescent patients may be a common source of infection among young adults. In addition, after primary EBV infection, virus may be intermittently shed in the saliva for life (3). It has been suggested that larger infectious doses of EBV that may be transmitted in saliva during kissing are responsible for the association of infectious mononucleosis with a history of sexual activity (22). Recently large studies of families in Denmark has suggested that genetic factors may predispose to developing infectious mononucleosis after EBV infection (126). Other studies of seroprevalence in the United States suggest that genetic and racial factors play a role in the likelihood of infection with EBV (160).
Oral Hairy Cell Leukoplakia
Oral hairy leukoplakia is an irregular white oral lesion, which is associated with active lytic replication of EBV in the lingual epithelium (134). It is not considered to be a premalignant condition. Oral hairy leukoplakia is mainly associated with advanced HIV infection, previously representing the second cause of oral lesions after candidiasis in this population (5). Some cases have also been described in other immunosuppressed populations, such as organ transplant recipients, but it is extremely uncommon in the immunocompetent host. Oral hairy leukoplakia is clearly related to the state of immunosuppression and CD4+ cell counts, and therefore, its incidence has decreased after the introduction of highly active antiretroviral therapy (117).
EBV-Associated Malignancies and Lymphoproliferative Syndromes
EBV-associated lymphoproliferative disease refers to the process of uncontrolled proliferation of EBV-infected B cells generally occurring in immunocompromised patients. The term post-transplant lymphoproliferative disorder (PTLD) is used when EBV-associated lymphoproliferation occurs after solid organ and hematopoietic stem cell transplantation (36). Post-transplant lymphoproliferative disorder is a heterogeneous entity whose clinical manifestations may range from a febrile process similar to infectious mononucleosis to an aggressive high-grade disseminated lymphoma (111). An in-depth treatment of this topic is provided in the chapter on post-transplant lymphoproliferative disorder.
EBV Lymphoproliferative Disease Associated with Primary Immunodeficiencies
Several rare genetic defects have been identified that lead to an inability to control EBV infections. These syndromes share a propensity for aggressive disease to develop upon primary EBV infection. Several are X-linked but others have recently been identified that are due to autosomal recessive mutations.
X-linked lymphoproliferative syndrome (XLP) is associated with a rare sex-linked genetic mutation that occurs with a frequency of less than 1 in 1 million males. X-linked lymphoproliferative syndrome is associated with a mutation in the S2HD1A gene that encodes SAP (SLAM-associated protein). SAP is expressed on T cells and is involved in intercellular communication and immune regulation (14). The exact relationship between SAP deficiency and inability to control EBV infection is not fully established but is likely due to defective NKT cell development (99, 107). As many as 4% of boys diagnosed with non-Hodgkin's lymphoma are found to have the mutant gene. Approximately 50% of X-linked lymphoproliferative syndrome cases appear to represent spontaneous mutations without a familial history.
A second type of X-linked lymphoproliferative syndrome is associated with mutations in the XIAP gene. This variant of X-linked lymphoproliferative syndrome (XLP and XLP2), is not associated with lymphoma development but is characterized by hemophagocytic lymphohistiocytosis (HLH) and colitis (76).
A syndrome of X-linked immunodeficiency with magnesium defect, EBV infection, and neoplasia, termed XMEN disease has recently been reported (78). X-linked immunodeficiency with magnesium defect, EBV infection, and neoplasia is caused by mutations in the gene encoding magnesium transporter 1 (MAGT1). Chronic high-level persistence of EBV-infected B cells, and heightened susceptibility to EBV-associated lymphomas are characteristic. The abnormality in intracellular magnesium homeostasis appears to lead to functional cellular immunodeficiency.
Deficiency of IL-2-inducible T-cell kinase (ITK) is associated with aggressive and fatal EBV-positive B cell proliferation and lymphoma. The ITK gene is located on chromosome 5 and the syndrome is therefore not X-linked. Lack of appropriate NK/T cell development is also characteristic of IL-2-inducible T-cell kinase deficiency (58).
Mutations in the perforin gene have been associated with familial hemophagocytic lymphohistiocytosis and with one case of chronic active EBV infection (64, 141).
Burkitt's Lymphoma
The endemic form of Burkitt lymphoma (BL) originally identified in sub-Saharan (equatorial) Africa is associated with EBV infection in >90% of cases and occurs in areas with a high incidence of malaria. The incidence of endemic Burkitt's lymphoma is estimated to be approximately 5-10 per 100,000. Endemic Burkitt's lymphoma is primarily a disease of children with a peak incidence in children less than 7. Sporadic Burkitt's lymphoma in the United States is less frequently EBV-associated (<25%) and is relatively rare with an age-adjusted incidence of approximately 0.3 per 100,000 person-years (95). Sporadic Burkitt's lymphoma primarily affects young adults. Burkitt's lymphoma occurs in 6 per 1000 cases of AIDS and EBV- positivity in HIV-associated Burkitt's lymphoma cases is variable (147).
Hodgkin's Lymphoma
Hodgkin's lymphoma is a lymphoma of B cell origin that occurs worldwide. Specific subtypes of Hodgkin's lymphoma, (mixed cellularity and lymphocyte-depleted), are more commonly associated with EBV infection. EBV-positive Hodgkin's disease may comprise up to 65% of all cases. It is now clear that not only is infectious mononucleosis a risk factor (RR=4.0) for the development of Hodgkin's lymphoma, but that infectious mononucleosis does not increase the risk of EBV-negative Hodgkin's disease. The median interval to the diagnosis of Hodgkin's disease after symptomatic infectious mononucleosis was 4.1 years in a large recent study (53).
AIDS-related Lymphoma (ARL)
AIDS-related lymphoma (ARL) refers to several types of lymphoma whose incidence is increased due to HIV-related immunosuppression. In addition to Burkitt's lymphoma, there is an increased incidence of several types of B cell lymphoma, which are EBV-related to varying degrees. Immunoblastic B cell lymphomas occur at much higher frequency in severely immunosuppressed patients, whereas Burkitt's lymphoma and diffuse large B cell lymphoma occur in the setting of higher CD4 counts. EBV infection plays a complex role in enhancing the survival of the infected B cell clones that give rise to lymphoma. In addition, primary effusion lymphoma (PEL) occurs almost exclusively in HIV-infected patients. Development of primary effusion lymphoma is tightly-associated to infection with Kaposi's sarcoma-associated herpesvirus (KSHV, HHV-8) but the majority of primary effusion lymphoma cells are also co-infected with EBV. CNS lymphoma is essentially 100% EBV-positive when it occurs in the setting of HIV infection whereas approximately 60% of peripheral B cell lymphomas in AIDS patients are EBV-associated.
Nasopharyngeal Carcinoma
Nasopharyngeal carcinoma is rare worldwide, with an incidence of less than one per 100,000, but occurs commonly in localized geographic regions in Southeast Asia and Africa with an incidence as high as 50 per 100,000 in some regions of Southern China (106). In addition to complex genetic susceptibility patterns, epidemiologic evidence implicates dietary factors such as the consumption of salted fish in the etiology of nasopharyngeal carcinoma (62, 162). Although EBV strain variation leading to particularly oncogenic variants has been suggested, firm evidence from molecular epidemiologic studies has not emerged.
EBV-positive Diffuse Large B-cell Lymphoma of the Elderly
EBV-positive diffuse large B-cell lymphoma of the elderly is an aggressive B cell neoplasm in immunocompetent adults characterized by varying degrees of EBV infection (102). Most cases occur in those >50 years of age and are more common in the Far East than in the US or Europe. The median age at presentation is 71 (range 50-91).
Lymphomatoid Granulomatosis
Lymphomatoid granulomatosis is a rare angiocentric and angiodestructive lymphoma derived from EBV-infected B cells (139). It is more common in males than females (2:1) and usually occurs after age 40-50. Various states of immunosuppression have been associated with lymphomatoid granulomatosis.
Chronic Active EBV Infection
EBV infection may lead to an aggressive infection with persistent and widespread organ involvement (16, 69, 70, 131). This rare manifestation most likely represents an inability of the host to adequately contain the primary infection and may reflect underlying specific immune deficits. Chronic active EBV infection is more common in Asia and South America than in the United States (57). Most cases have been reported from Japan where the median age at diagnosis is 8 years (range 1-50) compared to a mean age at presentation of 19 (range 4-51) in the United States. The type of cell infected also differs with Japanese and other non-US cases being virtually all due to EBV-infected T or NK cells. Cases from the United States have been primarily due to infected B cell proliferation, with fewer cases due to T or NK cells. An extensive spectrum of disease has been described, varying in clinical manifestations, severity and in the pathogenic role of EBV. The epidemiology of several of these syndromes is unique and differs based on geographic source as well as the type of syndrome. These may be broadly clinically categorized as chronic active EBV infection, hemophagocytic lymphohistiocytosis, mosquito bite hypersensitivity and hydroa vacciniforme-like lymphoproliferation (70). Since the classification of these syndromes is complex and there is considerable overlap in some aspects, the epidemiology of these syndromes will be further discussed in individual sections dealing with their clinical manifestations.

CLINICAL MANIFESTATIONS
Epstein-Barr virus is associated with a variety of clinical disorders arising from different pathogenic mechanisms (reviewed in 82). Infection during childhood is often asymptomatic or associated with nonspecific symptoms.
Infectious Mononucleosis
Infection during adolescence or adulthood more commonly results in the syndrome of acute infectious mononucleosis, characterized by a vigorous humoral and cellular immune response to rapidly proliferating EBV-infected B cells. Epidemiologic evidence suggests that the incubation period of infectious mononucleosis is greater than 4 weeks. Symptoms usually last 2-3 weeks and fever is present for up to two weeks, although symptoms of fatigue may persist for several weeks. The most common symptoms are sore throat, fever and lymphadenopathy. The exudative pharyngitis is often severe and associated tonsillar swelling can cause difficulty swallowing. Fever is almost universal, and lymphadenopathy is present in approximately 90% of patients at some point during the course of the illness. In a review of over 500 patients, lymphadenopathy was present in all patients, fever in 98 percent, and pharyngitis in 85 percent (54, 118). Headache, anorexia, malaise and fatigue are common. Fatigue may be persistent and severe. One prospective study of 150 patients found that most initial symptoms (e.g., fever, sore throat) had resolved by one month but fatigue resolved more slowly and persisted in 13 percent of patients for six months (118). Less common symptoms present in less than 25% of cases include parotitis, conjunctivitis and myalgias. Lymphadenopathy most commonly involves the posterior cervical than the anterior chains but can also be generalized. The enlarged nodes are mobile and only mildly tender. Lymphadenopathy occurs in the first week and then gradually subsides over two to three weeks. A rash that is usually non-pruritic is seen in less than 10% of patients. Administration of ampicillin, amoxicillin or less commonly, other drugs such as azithromycin (129), levofloxacin (105), piperacillin/tazobactam (77), and cephalexin (85) during the course of illness leads to a typical pruritic, maculopapular eruption that can be diffuse. The incidence of rash associated with beta-lactams was reported to be as high as 70 to 90 percent (56). Splenic enlargement is common and has been reported to be detectable by physical examination in 15-50% of patients in various studies. It usually occurs during the third week of illness (31). However, based on ultrasound examination, splenic enlargement is probably universal (X). Hepatic enlargement is less common and less prominent. Palatal enanthems and jaundice occur in less than 10-15% of patients. Asymptomatic elevations in transaminases occur in the majority of patients. Many aspects of this clinical syndrome, e.g. fever, lymphadenopathy, splenomegaly, atypical lymphocytosis, are due to the vigorous NK and T cell proliferation and cytokine response of the immune system rather than direct viral infection, replication, and cytolysis.
The syndrome of mononucleosis with atypical lymphocytosis can also be seen during primary infection with several other viruses including human cytomegalovirus, HIV, and Human Herpesvirus 6 (HHV-6), with CMV being the most common. Toxoplasmosis is another less common cause of a mononucleosis-like syndrome with lymphadenopathy.
Occasional serious and life-threatening complications of EBV infection occur and include autoimmune hemolytic anemia, hemophagocytic syndrome, thrombocytopenia, splenic rupture, airway obstruction and neurologic syndromes (137). Thrombocytopenia is common but usually not severe enough to cause a bleeding diathesis although rare cases of fatal hemorrhage associated with primary EBV infection have been reported. Palatal petechiae, however, are common and observed in approximately 10% of patients with IM. While asymptomatic mild hepatitis is common, severe liver involvement with elevation of bilirubin may occur, but is usually self-limited.
Several neurologic complications of primary EBV infection occur and include both peripheral and central nervous system syndromes. CNS manifestations include encephalitis, Bell's palsy, central and peripheral neuropathies, transverse myelitis and meningoencephalitis. Guillain-Barre syndrome has been reported as a complication of EBV infection and typically presents with facial or peripheral paresthesias followed by weakness of the extremities, which may be progressive. The Miller Fisher variant of Guillain-Barre syndrome, characterized by a descending paralysis, ophthalmoplegia, areflexia and ataxia has also been reported. Encephalitis and cerebellitis may be the initial presentation of EBV infection, particularly in children, and may occur despite a negative Monospot test. Several of the neurological manifestations of EBV infection, including Guillain-Barre syndrome, polyradiculomyelitis and transverse myelitis, appear to be post-infectious in nature rather than due to infection and replication of EBV in affected tissues. The vast majority of patients (approximately 85%) with EBV-associated neurological complications recover without permanent sequelae.
Splenic rupture is a rare but potentially life-threatening complication of IM. It is spontaneous in more than one-half of cases, with no history of specific injury. Rupture often occurs between the second and third week of illness (42). Despite its life-threatening potential, fatality is rare. Nonoperative treatment with intensive supportive care and splenic preservation has been successfully carried out in some cases, while others require splenectomy (118). Airway obstruction due to massive lymphoid hyperplasia and mucosal edema is an uncommon and potentially fatal complication. Severe obstruction can be successfully treated by tracheotomy or endotracheal intubation. The use of corticosteroids to reduce pharyngeal edema and lymphoid hypertrophy is suggested for individuals with airway obstruction. Neurologic complications are rare and include encephalitis, Guillain-Barre syndrome, facial nerve palsy, transverse myelitis, peripheral neuritis, and optic neuritis (129). "Alice-in-Wonderland" syndrome is a visual illusion manifested as a distortion in size, form, movement, or color. Onset may occur during or soon after the resolution of the clinical symptoms of infectious mononucleosis, and it may resolve within 4 to 6 weeks. Visual-evoked potentials suggest diminished cerebral perfusion in affected cases (74).
Oral Hairy Leukopenia
Oral hairy leukoplakia (OHL) is a benign white lesion most commonly seen on the lateral surface of the tongue and occasionally on the dorsal surface. The lesions actually have a corrugated, rather than a hairy appearance and present as white patches. Oral hairy leukoplakia is almost exclusively seen in patients with HIV infection and occasionally in patients with other types of chronic immunosuppression. The lesions are asymptomatic and symptoms, when they occur, are attributable to irritation of the lesion. No malignant transformation has been observed, and oral hairy leukoplakia is not considered a pre-malignant lesion. Oral hairy leukoplakia lesions are not friable and the main differential diagnosis is oral candidiasis.
Chronic Active EBV and Related Syndromes (Hemophagocytic Lymphohistiocytosis, Hypersensitivity to Mosquito Bites and Hydroa Vaccinniforms-like Lymphoproliferative Disease)
Rare patients have an unusual clinical course following infectious mononucleosis and develop a chronic active infection characterized by ongoing symptoms, persistent or recurrent fever and lymphadenopathy and involvement of multiple sites, including neurologic, pulmonary, gastrointestinal, hepatic, cardiac and ocular organ systems (131). Unlike the pattern in most EBV-associated diseases, infection of NK and T cells occurs commonly in chronic active EBV infectionand may result in T or NK cell lymphoproliferative disease or lymphoma. While chronic active EBV infection in Japan and other areas of Asia and South America is typically exclusively due to proliferation of EBV-infected T and NK cells and chronic active EBV infection in the United States is more often due to EBV infection of B cells, the clinical course is similar in both types of disease. Progression to lymphoma is common in both types of chronic active EBV infection. These patients may have extremely high antibody responses to EBV several lytic proteins, lack antibodies to EBNA-1, and exhibit severe disease with end organ involvement. Evidence of increased expression of EBV DNA, RNA or protein may be detected in affected tissues and peripheral blood (16, 70, 90, 131, 142). In the United States cases due to B cell infection, progressive depletion of B cells and hypogammaglobulinemia was observed (16). Chronic active EBV infection in Japan and other Asian countries has been reported to have different characteristics depending on whether T or NK cells are affected. There was a trend to better survival in patients with NK cell infection versus those with infected T cells (70). Fever and high titers to EBV antigens was also more common in T cell chronic active EBV infection.
Three other related syndromes have been characterized in the Japanese population who have T/NK cell EBV infection, suspected lymphoproliferative disorder, high EBV viral load and no other immunodeficiencies. These are hemophagocytic lymphohistiocytosis, hydroa vacciniforme-like lymphoproliferative disease and severe mosquito bite "allergy" (SMBA) (70). Patients with hemophagocytic lymphohistiocytosis present with fever, generalized lymphadenopathy, hepatosplenomegaly, hepatitis, pancytopenia and coagulopathy (27). The syndrome is characterized by generalized histiocytic proliferation and hemophagocytosis (148). Patients with hypersensitivity to mosquito bites frequently present in childhood with abnormal responses to mosquito bites that is not an allergic reaction but an abnormal cutaneous reaction consisting of necrosis accompanied by NK cell lymphocytosis and systemic symptoms. Hydroa vacciniforme-like lymphoproliferative disease is now recognized as a chronic EBV-associated lymphoproliferative disorder with a propensity to develop lymphoma (24). Cases present in childhood with vesiculopapular lesions that progress to ulceration and scarring in both sun-exposed and non sun-exposed areas. Fever, lymphadenopathy and hepatosplenomegaly may be present, and elevated EBV loads in PBMCs are frequently observed. Progression to frank lymphoma is common but not universal (115). In the most extensive study of chronic active EBV infection and related syndromes in the Japanese population, hemophagocytic lymphohistiocytosis was defined as meeting clinical criteria of fever and splenomegaly, laboratory criteria of cytopenia in 2 lineages in peripheral blood, hypertriglyceridemia and/or hypofibrinogenemia and histological evidence of hemophagocytosis. Hemophagocytic lymphohistiocytosis as a component of accelerated chronic active EBV infection was excluded. Severe mosquito bite "allergy" was defined as hypersensitivity to mosquito bites characterized by high fever after bites, ulcers, necrosis, and scarring. Hydroa vacciniforme was defined as recurrent vesiculopapules with central umbilication and crust formation mimicking herpetic vesicles usually occurring on sun-exposed areas. The cell type infected in each of these syndromes was distinct. Whereas infected cells in chronic active EBV infection was approximately 60% T cells and 40% NK cells, 53% of hemophagocytic lymphohistiocytosis patients had CD8+ T cell infection, a cell type rarely seen in the other conditions. The majority of severe mosquito bite "allergy" patients, 89%, had NK cell infection and 75% of HV patients had gd T cell infection.
X-Linked Lymphoproliferative Disease
Individuals with a rare, inherited X-linked immunodeficiency known as X-linked lymphoproliferative syndrome or Duncan's syndrome, are at risk for overwhelming lethal primary infection with Epstein-Barr virus (10, 114). The clinical presentation is that of a fulminant infectious mononucleosis syndrome with typical and severe symptoms of infectious mononucleosis. In addition, patients often develop a severe hepatitis usually culminating in fatal hepatic failure. Patients may also develop erythrophagocytic syndrome. Survivors are at risk for the subsequent development of lymphoma and dysgammaglobulinemia. The genetic defect in these patients has been mapped to a small cytoplasmic protein SAP, implicated in regulation of T and NK cell signaling (13). Genetic defects in the SAP gene lead to a defect in the development of NK and T cells in both mice and humans, suggesting a mechanism for the development of deficient antiviral responses (12, 99).
EBV Associated Malignancies
Burkitt's Lymphoma
Burkitt's lymphoma usually presents with lymphadenopathy or an abdominal mass and is much more common in children than in adults. The endemic African form of Burkitt lymphoma typically presents in the jaw and the orbit. Burkitt lymphoma is an extremely rapidly-growing tumor and disseminated disease involving bone marrow and CNS is common (15-40%). Almost all patients with sporadic Burkitt's lymphoma have abdominal tumors with a high incidence of bone marrow involvement. Presentation in HIV patients is variable and often includes lymphadenopathy. High levels of serum lactate dehydrogenase (LDH) are usually seen secondary to a high degree of cell lysis. It should be emphasized that rapid diagnosis and treatment of Burkitt lymphoma is extremely important as the response and cure rate is greater than 70% with appropriate initial therapy whereas salvage therapy is markedly less successful.
Hodgkin's Lymphoma
Hodgkin's lymphoma usually presents as lymphadenopathy. Affected lymph nodes are hard, non tender, and asymmetric. In 75% of the cases the first localization of lymphadenopathy is cervical. Mediastinal adenopathy occurs in over 50% of patients and B symptoms such as fever and weight loss are common. In Hodgkin disease dissemination to spleen and liver is frequently seen, but an extra-lymphatic localization is uncommon. Hodgkin's lymphoma has also been associated with a large variety of unusual paraneoplastic manifestations including skin or CNS abnormalities, (pruritus, Guillain-Barré syndrome), nephrotic syndrome, hemolytic anemia and thrombocytopenia. Hodgkin's lymphoma has a very high cure rate and relapses have been successfully treated with intensive chemotherapy and stem cell transplantation.
Nasopharyngeal Carcinoma
Nasopharyngeal carcinoma of the undifferentiated type is essentially 100% EBV-associated. As mentioned earlier, this type of nasopharyngeal carcinoma is common in Southeast Asia and is also found in Northern African and Inuit populations but is rare in other geographic areas except in immigrant populations. The initial clinical manifestations are usually headache, nasal obstruction and otitis media, but a proportion of patients may remain asymptomatic for long periods of time (156). Therefore, diagnosis is often delayed and patients may present with metastatic head and neck masses, or with basal skull invasion and cranial nerve paralysis.
Nasopharyngeal carcinoma is also associated with paraneoplastic syndromes, such as hypertrophic osteoarthropathy and the syndrome of inappropriate secretion of antidiuretic hormone (SIADH). Serological screening of high-risk populations for IgA antibodies against VCA and early antigen allows identification of early cases for close monitoring. Definitive diagnosis requires endoscopic biopsy and demonstration of EBV antigen or Epstein-Barr virus-encoded RNA (EBER) expression in malignant tissue. Endoscopic brushing with measurement of EBV DNA load and specific EBV mRNAs expressed in tumors may allow less invasive diagnostic testing and follow-up (136).
AIDS-Related Lymphoma
EBV-associated AIDS-related lymphoma other than Burkitt's lymphoma and HD are primarily diffuse large B cell lymphomas and primary CNS lymphomas that may differ from their presentation in HIV-negative patients. The majority of diffuse large B cell lymphomas present as asymptomatic or symptomatic lymphadenopathy with or without associated constitutional symptoms. Symptoms from lymphadenopathy are usually due to compression of adjacent structures. Clinical manifestations of primary CNS lymphoma in HIV positive patients are those of a brain mass. Therefore, the differential diagnosis of CNS lymphoma in this population includes toxoplasmosis, pyogenic brain abscess, and nocardiosis, among others.
EBV-Positive Diffuse Large B-cell Lymphoma of the Elderly
While clinical aspects of EBV-positive diffuse large B-cell lymphoma of the elderly are similar to diffuse large B-cell lymphoma in general, overall prognosis is generally poorer. Extranodal involvement is common, and EBV infection may correlate with poorer outcome, particularly in Asian patients.
Lymphomatoid Granulomatosis
Lymphomatoid granulomatosis is characterized primarily by pulmonary involvement, with symptoms of dyspnea, cough and hemoptysis. The skin and nervous system are commonly involved, with occasional involvement of other organs. Systemic symptoms such as fever and weight loss are also reported. While it may be clinically mistaken for granulomatosis with polyangiitis (GPA), renal involvement is less common, and histopathology reveals infiltration of blood vessels by proliferating EBV-positive lymphocytes. Necrosis of the lymphoid aggregates (granulomatosis) is seen rather than the chronic inflammation and granuloma formation typical of autoimmune vasculitis such as granulomatosis with polyangiitis.
Diffuse Large B-Cell Lymphoma
Diffuce large B-cell lymphoma arising in the setting of chronic inflammation typically presents with respiratory symptoms, chest or back pain and fever with swelling at the site of the tumor (97). The majority of cases reported have been in the setting of prior pyothorax and tuberculosis. EBV-positive diffuse large B-cell lymphoma with chronic inflammation has also been reported in association with metallic implants and other prosthetic devices. Most cases are of B cell origin and tend to be located in the pleura with local invasion. Despite presentation at lower stages, the clinical course is aggressive. The pattern of EBV gene expression (type III) is similar to that seen in post-transplant lymphoproliferative disorder (PTLD) and other highly immunosuppressed states, with expression of several EBV latent antigens, suggesting that long-standing perturbations in local immunity at the site of chronic inflammation allow outgrowth of malignant clones.
LABORATORY DIAGNOSIS
Laboratory confirmation of EBV infection is primarily achieved by serological testing. Heterophile antibodies directed against sheep erythrocyte agglutinins are positive in about 90% during the primary infection. Commercially available Monospot testing for heterophile antibodies is less sensitive in children and sequential Monospot testing or determination of EBV-specific antibodies is indicated when the clinical findings are suggestive of EBV infection but the initial Monospot is negative.
In the clinical setting in which the young adult patient has typical infectious mononucleosis, a Monospot will confirm the diagnosis in more than 90% of cases. Unless the history suggests the possibility of other infections such as HIV, a battery of viral serologies is not routinely necessary. If the presentation is atypical but suggestive of infectious mononucleosis, and the Monospot is negative, EBV serology can confirm the diagnosis or indicate whether testing for other pathogens such as CMV, toxoplasmosis may be appropriate, based on the clinical presentation and history.
The presence of IgM antibodies to viral capsid antigen (VCA) is the most sensitive and specific indicator of acute infection (Table 1). These are usually detectable at the initial presentation, along with IgG VCA Abs. IgM VCA antibodies, however, decline and are absent by 4-8 weeks, whereas IgG VCA Abs persist for life (28, 56). Therefore, IgG VCA antibodies are not usually useful for establishing the presence of active EBV infection since virtually all patients are IgG positive by the time they seek medical attention. Testing for the presence of IgM VCA antibodies and the absence of antibodies to Epstein-Barr nuclear antigen (EBNA) is useful for identifying active and recent infections. Because antibodies to Epstein-Barr nuclear antigens do not develop until approximately 4 weeks after onset of symptoms and persist for life (49), seroconversion to anti-EBNA positivity is therefore indicative of recent EBV infection. Although antibodies to EBV early antigens are often elevated during acute infection, they may persist for variable periods and are occasionally detectable in healthy convalescent patients many years after infection, and are therefore of limited utility in diagnosing acute infection (56). The patterns of antibody responses to EBV infection are illustrated in Figure 1.
At the time of presentation, VCA IgM antibodies are positive, and VCA IgG and early antigens are also usually positive. As convalescence proceeds, Epstein-Barr nuclear antigen (EBNA) antibodies become detectable and VCA IgM disappears. EBNA and VCA IgG antibodies remain detectable for life and early antigen antibodies are also usually detectable though at low titers. The amount of EBV DNA in blood or plasma, quantified through polymerase chain reaction (PCR) assays, can also be used for diagnosing symptomatic EBV infection (157). One study evaluated the clinical utility of detecting EBV viremia with real-time PCR in children with primary EBV infection compared to controls (108). Within the primary infection group, those with detectable virus were more likely to have lymphadenopathy, higher atypical lymphocytes counts, and higher aminotransferases than those without detectable virus. It has also been shown that in a patient with IM, the virus load decreased as the symptoms resolved (71). Figure 2 shows the changes of the virus load in a patient with IM. Generally speaking, however, EBV viral load testing in peripheral blood provides little information over serology in the immunocompetent patient being neither sensitive nor specific as a test for primary infection. However, it may be useful in situations where chronic active EBV infection is suspected or the serology results are ambiguous.
The diagnosis of oral hairy leukoplakia is usually made clinically based on the appearance of the lesion in an appropriate clinical setting and biopsy is generally unnecessary. When biopsies are performed, they are positive for EBV genomes by in situ hybridization and EBV gene expression by immunofluorescent staining. There are also histopathologic changes characteristic of oral hairy leukoplakia, including perinuclear halo formation (koilocytic cells), hyperparakeratosis and acanthosis (increased thickness of the stratum spinosum).
PATHOGENESIS
After resolution of primary infection, EBV persists for life as a latent infection in 1/104 to 1/106 memory B cells. Persistent EBV infection is controlled by a virus-specific immune response and is asymptomatic in most humans. However, immunosuppression associated with HIV infection, transplantation, or congenital immunodeficiencies can result in uncontrolled oligoclonal or monoclonal B cell proliferation of latently infected cells. Uncontrolled lytic infection in the oropharynx is manifested as oral hairy leukoplakia in immunosuppressed hosts (38) but manifestations of virtually all other lymphoproliferative and malignant diseases associated with EBV are due to latently infected cells. The oncogenic role of EBV in the various conditions discussed above ranges from a direct proliferative and anti-apoptotic stimulus provided by EBV proteins in a setting of immunodeficiency (as in post-transplant lymphoproliferative disorder ) to a cofactor that predisposes to the development of a lymphoma which is no longer continuously dependent on the expression of EBV gene products.
It has been reported that patients who experience infectious mononucleosis as a consequence of primary infection may have a long-lasting and possibly permanent down-regulation of the IL-15 receptor IL15Rα on T and NK cells, resulting in potential long-term effects on immunologic function (127). However, a more recent study challenges this finding, and suggests that selective and long-term effects on immune function are unlikely (34).
The pathogenesis of EBV-associated disease is closely correlated with the proliferative stimulus of EBV on the infected cell and the immune status of the host. The pattern of EBV latent gene expression in each EBV-associated disease is distinct (1). Many of the proteins expressed by EBV have been identified as having either growth-promoting, anti-apoptotic or immune evasion function. EBV may also rescue B cells during germinal center maturation, providing non-physiologic survival signals that predispose to subsequent development of B cell malignancy. Vaccination, immunomodulation, or pharmacologic intervention of important cell-signaling pathways usurped by viral gene products might provide more effective therapeutic strategies against EBV-associated malignancies than traditional anti-viral drugs designed to block viral replication.
SUSCEPTIBILITY IN VITRO AND IN VIVO
Because EBV infection typically results in latent infection, rather than a lytic infection associated with plaque formation, EBV sensitivity to conventional antiviral drugs cannot be assayed by conventional plaque reduction assays. Instead, latently infected cell lines are used in which cells can be induced for lytic viral replication in the presence or absence of potential antiviral agents. Antiviral activity is measured by quantifying viral DNA and is expressed as the concentration of drug required to inhibit 50% of viral DNA replication induced by lytic infection (IC50). Using these types of assays, acyclovir has an IC50 of 0.3 μM for EBV, and ganciclovir has an IC50 of 0.05 μM for EBV (18, 66, 79). Both drugs require initial phosphorylation by a viral kinase to be subsequently incorporated into DNA and terminate viral DNA replication. It was originally thought that acyclovir was phosphorylated by an EBV-specified thymidine kinase. Subsequent discovery of an EBV protein kinase led to controversy over which kinase is responsible for acyclovir and ganciclovir phosphorylation, but it appears that in infected cells, the EBV protein kinase is the enzyme required for activity of acyclovir and ganciclovir (87). The conserved mechanisms of lytic replication among herpesviruses suggests that other antiviral drugs developed against herpes simplex or cytomegalovirus replication may have activity against EBV lytic infection.
Despite the effectiveness of acyclovir against EBV lytic replication, acyclovir has no inhibitory activity on replication of the episomal EBV genomes present in latent infection. Thus, acyclovir will inhibit production of linear genomes in the minority of cells entering lytic infection in an EBV-infected B cell line, but episomal DNA is replicated by cell DNA polymerases and is unaffected by acyclovir in latently EBV-infected B cells. Once acyclovir is removed, lytic replication can resume from the latent EBV genomes (17, 103). Thus, immortal B cell growth induced by latent EBV infection is unaffected by acyclovir treatment in vitro, and these in vitro studies are consistent with the clinical experience that nucleoside analogues have little effect on EBV-induced malignancies associated with latent EBV infection. Acyclovir may have some marginal utility in some situations in highly immunocompromised hosts by preventing ongoing production of infectious virions and infection of additional B cells, thereby leading to expansion of the reservoir of infected cells.
ANTIVIRAL THERAPY
Infectious mononucleosis
The issue of whether nucleoside analogues might be effective during primary gammaherpesvirus infection, where viral replication is more likely to play an important pathogenic role, has been extensively studied in infectious mononucleosis. In 6 different studies involving a total of approximately 320 patients, oral or intravenous acyclovir therapy consistently reduced or eliminated lytic EBV infection during therapy as detected by virus shedding in oropharyngeal secretions but had no effect on clinical outcome, duration of symptoms, or establishment of persistent infection in the oropharynx or peripheral blood B lymphocytes (3, 4, 104, 153, 154, 161). Further, one meta-analysis of five randomized controlled trials of acyclovir in the treatment of acute IM, including two trials of intravenous therapy in patients with severe disease, also failed to show a clinical benefit compared to placebo (152). Thus, acyclovir can effectively inhibit lytic EBV replication in vivo, but acyclovir treatment initiated after the onset of symptoms has no clinical benefit in infectious mononucleosis. These results are not surprising since latent infection has already been established and the vigorous host immune response to virus infection responsible for the majority of symptoms has been triggered. In rare, complicated cases of primary EBV infection and infectious mononucleosis where the patient is immunosuppressed or severely ill, acyclovir or ganciclovir treatment may be rational given the safety profile of these drugs, their ability to inhibit EBV replication in vitro and in vivo, and anecdotal reports of clinical response in unusual cases where excessive EBV replication may have been pathogenic (20, 54, 86, 111).
Oral Hairy Leukoplakia
Oral hairy leukoplakia is an unusual lesion of the tongue found in HIV-infected patients. Vigorous EBV lytic replication is present in the excessively proliferating epithelium. This is the only instance where disease appears to be a direct consequence of lytic EBV replication, and oral acyclovir therapy (3.2 gm/day) can temporarily reverse the lesions (119). However, lytic EBV replication and oral hairy leukoplakia generally recur upon withdrawal of therapy and the mainstay of treatment is antiretroviral therapy directed against HIV. Successful treatment of the underlying immunosuppression usually results in resolution of oral hairy leukoplakia. Treatment of associated oral candidiasis or CMV infection may also be necessary.
EBV-Induced Lymphoproliferations Associated With Immunosuppression
The role of antiviral therapy against EBV for the treatment of EBV-associated post-transplant lymphoproliferative disorder has not been fully established. The most common antiviral drugs used, i.e. acyclovir and ganciclovir (or their pro-drugs), act by inhibiting the DNA polymerase in EBV-infected lytic cells. Since the lymphoproliferative process is driven primarily by latent EBV gene products, the utility of antiviral therapy is unclear. Thus antiviral therapy is unlikely to be of benefit in the lymphoproliferative disorders in which immunosuppression may play a role such as EBV-positive diffuse large B-cell lymphoma in the elderly or lymphomatoid granulomatosis. Phase II/III clinical trials are underway to assess the feasibility of chemically inducing lytic gene expression in the proliferating EBV-infected cells in lymphoproliferative disease and killing the induced cells with ganciclovir. Specifically, EBV kinase expression may be induced in EBV-infected cells by treatment with arginine butyrate, rendering the cells susceptible to killing by ganciclovir (88). (Please see http://www.cancer.gov/clinicaltrials for details of these and other active trials).
EBV-Associated Hemophagocytic Lymphohistocytosis
Antiviral therapy is not effective. Treatment consists of immunomodulatory and cytotoxic protocols specifically directed to control of hemophagocytic lymphohistiocytosis in both EBV-associated and hemophagocytic lymphohistiocytosis due to other causes (See below under adjunctive therapy).
Chronic Active EBV Infection
Both clinical responses and failures with acyclovir or corticosteroids have been noted in anecdotal reports of these rare patients with chronic active EBV infection (131, 143). As described earlier, however, antivirals did not seem to have significant effects in either Japanese or American patients with chronic active EBV infection (16, 70). A placebo controlled study with acyclovir has shown no efficacy for patients with chronic fatigue syndrome (144).
EBV-Associated Malignancies
There is no proven effective antiviral therapy for the Burkitt's lymphomas, nasopharyngeal carcinoma, and Hodgkin's lymphoma associated with EBV infection, and treatment is usually based upon cancer chemotherapy. However, trials are also underway combining bortezomib, a proteasome inhibitor shown to induce apoptosis in EBV-transformed B cells (163), and ganciclovir in the treatment of relapsed or refractory EBV-positive lymphoma. Adoptive transfer of EBV-specific cytotoxic T lymphocytes may also be useful for treating these types of EBV-associated malignancies and a variety of trials utilizing this approach are also open for enrollment at the time of this edition. Boosting of the immune response to EBV latent antigens by expressing these genes in dendritic cells may offer promise for treatment of relapsed Hodgkin's lymphoma (33). Novel pharmacologic approaches against latent EBV infection may be another approach for treating these diseases. Antisense oligonucleotides may be used to disrupt specific essential latent gene functions, such as EBNA-1 binding and maintenance of the latent EBV episome (67). Delineation of the cell signaling pathways used by EBV latent genes, such as the tumor necrosis factor receptor pathway by LMP1 (96), may provide unique opportunities to block virus induced cell proliferation or to induce apoptosis of virus infected cells.
ADJUNCTIVE THERAPY
Infectious Mononucleosis
Supportive treatment is generally indicated since more than 95% of infectious mononucleosis cases resolve uneventfully without specific therapy. Acetaminophen can be used to reduce fever. Use of concomitant antibiotics for possible bacterial pharyngitis should be judicious and supported by positive culture results due to the high incidence of allergic reactions to antibiotics such as ampicillin during acute infectious mononucleosis.
The use of corticosteroids for uncomplicated infectious mononucleosis is still controversial. Corticosteroids have been shown to reduce fever and shorten the duration of constitutional symptoms (11, 19, 72, 113, 132). However, adverse drug complications can arise from even short courses of corticosteroid use (17, 157), and corticosteroid use is probably best avoided for routine infectious mononucleosis, a self-limited disease. Corticosteroid use is generally reserved for infectious mononucleosis cases complicated by potential airway obstruction from enlarged tonsils, severe thrombocytopenia, or severe hemolytic anemia (21, 113, 137). These complications result from the excessive immune response to virus infection rather than uncontrolled viral infection, and a short course of corticosteroids at 1 mg/kg/day of prednisone with tapering over 1-2 weeks can be effective for treating the excessive tonsillar proliferation or autoimmune symptoms. Corticosteroids might also be used for other autoimmune complications rarely associated with infectious mononucleosis such as CNS involvement, myocarditis or pericarditis (86). Unless contraindicated, it is our general practice to administer acyclovir concurrently with corticosteroids.
Splenic rupture is a rare but potentially fatal complication of infectious mononucleosis and occurs in approximately 0.1% of cases of infectious mononucleosis (6, 30). Splenic rupture is more common in males and approximately half the cases are spontaneous (not associated with trauma or other contributory factors). In one review of 55 cases of infectious mononucleosis-associated splenic rupture, all cases occurred within three weeks after the beginning of illness. Another case-control study which combined physical, ultrasound and laboratory examinations of infectious mononucleosis patients found that physical examination was an insensitive method of detecting splenomegaly (17%), but all patients were found to have splenomegaly for the first 20 days, and the severity of laboratory abnormalities did not correlate with splenic enlargement (26). Although various strategies to minimize the risk of splenic rupture have been advanced, incorporating the results of physical exam and ultrasound imaging, no studies have validated the utility of such approaches. It therefore seems prudent to recommend avoidance of contact sports or activities that raise intra-abdominal pressure such as weight lifting for a minimum of four weeks after the onset of illness.
Patients recovering from infectious mononucleosis may shed high titers of EBV in saliva for periods of several months after recovery despite being clinically well (See Epidemiology above). Furthermore, it is clear that all latently infected humans may intermittently shed EBV in saliva. It is therefore difficult for seronegative subjects to avoid the risk of acquiring EBV infection. It appears that intimate sexual contact is more likely to transmit EBV infection.
Chronic Active Epstein-Barr Virus Infection (CAEBV)
Treatment of chronic active EBV infection with a variety of approaches has been attempted in both the United States and in Japan. While the syndromes vary considerably by geographic location, the responses to treatment have been similar. The most effective intervention in both T/NK and B cell disease appears to be allogeneic hematopoietic stem cell transplant (HSCT). While the reported numbers in the United States are small, there was a 63% survival rate in those receiving a hematopoietic stem cell transplant (16). Similar results have been reported from Japan, with improved survival in approximately 66% of patients who received a hematopoietic stem cell transplant (70). In both series, treatment with antivirals, cytokines, immunoglobulin, rituximab or conventional chemotherapy led to either transient improvement or had no effect. Treatment with rituximab has been associated with the emergence of CD20-negative malignant clones (16). In patients with hemophagocytic lymphohistiocytosis alone, immunomodulatory therapy was temporarily effective but did not prevent progression in those with chronic active EBV infection. In general, there was a trend to improved outcome with earlier transplantation. Infusion of EBV-specific allogeneic donor T cells appeared to have a useful role post-transplantation, decreasing or eliminating persistent detectable EBV in the peripheral blood. Recently, investigators have successfully treated EBV-induced lymphoproliferative disease by augmenting the host's immune response through adoptive transfer of EBV-specific cytotoxic T cells grown in vitro (124, 125). Donor T cells are harvested prior to transplantation and stimulated in vitro with an EBV-infected B cell line prior to infusion into the recipient. These cytotoxic T lymphocytes amplify in vivo and persist long-term.
EBV-Associated Hemophagocytic Lymphohistocytosis
The aim of therapy is suppression of the increased inflammatory response and control of T cell proliferation using immunosuppressive and cytotoxic drugs. Chemotherapy using dexamethasone, cyclosporin A, and etoposide is used for severe EBV-associated hemophagocytic lymphohistiocytosis cases (50).
X-Linked Lymphoproliferative Disease
Hematopoietic stem cell transplantation performed during childhood with HLA-identical sibling donors, regardless of EBV serologic status, offers potentially curative therapy for X-linked lymphoproliferative disease (39).
EBV-Associated Malignancies (Burkitt's Lymphoma, Nasopharyngeal Carcinoma, Hodgkin's lymphoma, ARL)
The usual treatment for EBV-associated malignancies is based on cancer chemotherapy and radiation therapy as opposed to antiviral strategies. As mentioned above, the progression of some of these malignancies can be extremely rapid and referral to a specialized oncology center is essential for prompt diagnosis, staging, and appropriate initial therapy.
The treatment of AIDS-related lymphoma is complicated by the presence of HIV coinfection and the interaction of immunosuppression, drug interactions and side effects of both antiretroviral therapy and chemotherapy directed against lymphoma. Although initial trials indicated that HAART could be successfully co-administered with chemotherapy, additional trials in which HAART was suspended during chemotherapy were carried out. These trials, which used dose-adjusted multi-modality chemotherapy (DA-EPOCH) found that although HIV loads did increase during HAART suspension, HIV control was achieved by resumption of HAART (80). While this study did indicate that HAART could be suspended during chemotherapy, current reports support the feasibility and possible advantages of continuing HAART during chemotherapy (2). A second unresolved issue in the treatment of AIDS-related lymphoma is the risk versus benefit of rituximab in addition to CHOP chemotherapy in AIDS patients. Although rituximab improved lymphoma response in a multi-center trial of EBV-positive diffuse large B-cell lymphoma (DLBCL) in HIV patients, overall survival was not improved due to an increase in treatment-related infections in the rituximab group (56). However, several investigational trials using dose-modified regimens that included rituximab in both AIDS-related EBV-positive diffuse large B-cell lymphoma and Burkitt's lymphoma suggest high efficacy despite significant toxicity (120, 160). The optimal balance between efficacy and safety remains to be established.
VACCINES
Potential strategies for EBV vaccination include prophylactic approaches (to prevent infection or attenuate morbidity associated with primary infection/infectious mononucleosis), post-infection approaches (to reduce or eliminate persistent EBV infection and risk of EBV-associated malignancies), and therapeutic approaches (to treat established EBV-infected malignancies). Most work has focused on the EBV major membrane glycoprotein, gp350, as a potential EBV vaccine (94). EBV binding to the cellular receptor, CD21, is mediated by gp350 (98), and a gp350 subunit vaccine can prevent the development of lymphomas after injection of EBV in a cotton-top tamarin animal model for EBV infection (92, 93, 116). A small trial with a recombinant gp350 vaccinia virus vaccine showed that it can induce EBV neutralizing antibodies in human volunteers. However, 3/9 vaccinated volunteers with neutralizing antibody were subsequently infected with EBV by natural routes of transmission (40). A recently completed phase II trial showed that the EBV gp350 subunit vaccine was associated with a decreased risk of infectious mononucleosis in a cohort of healthy seronegative subjects. IM occurred in 2 of 90 patients in the vaccine group and 8 of 91 in the placebo group (138). Interestingly, asymptomatic infection occurred in 11 and 9 subjects in the vaccine and placebo group, respectively, suggesting that the vaccine may not reduce the likelihood of asymptomatic infection.
More studies will be required to determine the role of humoral versus cellular immunity, the importance of mucosal immunity, the optimal adjuvant and delivery system for gp350 vaccines, and whether a gp350 vaccine will decrease the increased risk of malignancy associated with EBV infection. In this regard, attenuation rather than prevention of infectious mononucleosis by the vaccine may be sufficient to decrease the risk of malignancy such as Hodgkin's lymphoma, which is associated with severe primary infection. It remains to be determined whether gp350 represents the optimal candidate for an EBV vaccine. Vaccines that induce cytotoxic T cell activity against EBV latent genes have also been proposed as a potentially effective vaccine strategy. Preliminary trials in volunteers using synthetic peptides of multiple fused EBV cytotoxic T lymphocyte epitopes are also underway (68). An animal model in rhesus monkeys that reproduces the natural route of oral transmission and other aspects of acute and persistent EBV infection has recently been established and the complete sequence of the rhesus EBV homolog has been determined (91, 123). These advances should be useful for the development of effective EBV vaccine strategies.
REFERENCES
1. Alfieri C, Birkenbach M, Kieff E. Early events in Epstein-Barr virus infection of human B lymphocytes. Virol 1991;181:595-608. [PubMed]
2. Alwan F, He A, Montoto S, Kassam S, Mee M, Burns F, Edwards S, Wilson A, Tenant-Flowers M, Marcus R, Ardeshna KM, Bower M, Cwynarski K. Adding Rituximad to Codox-M/IVAC chemotherapy in the treatment of HIV-associated Burkitt Lymphoma is safe when used with concurrent combination antiretrovial therapy. 2015 May 15;29(8):903-10. [PubMed]
3. Andersson J, Ernberg I, Andersson U, Henle W, Skoldenberg B, Tisell A. Effect of acyclovir on infectious mononucleosis: a double-blind, placebo-controlled study. J Infect Dis 1986;153:283-90. [PubMed]
4. Andersson J, Henle W, Giesecke J, Ortqvist A, Julander I, Gustavsson E, Akerlund B, Britton S, Ernberg I. Acyclovir treatment in infectious mononucleosis: a clinical and virological study. Infection 1987;15:Suppl.1:S14-20.[PubMed]
5. Arendorf TM, Bredekamp B, Cloete CA, Sauer G. Oral manifestations of HIV infection in 600 South African patients. J Oral Pathol Med. 1998; 27: 176-179.[PubMed]
6. Asgari MM, Begos DG. Spontaneous splenic rupture in infectious mononucleosis: a review. Yale J Biol Med 1997;70:175-82. [PubMed]
7. Babel N, Vergopoulos A, Trappe RU, et al. Evidence for genetic susceptibility towards development of posttransplant lymphoproliferative disorder in solid organ recipients. Transplantation. 2007; 84: 387-391. [PubMed]
8. Balfour HH, Jr. Editorial commentary: Genetics and infectious mononucleosis. Clin Infecrt Dis 2014;58:1690-1. [PubMed]
9. Balfour HH, Holman CJ, Hokanson KM, Lelonek MM, Giesbrecht JE, White DR, Schmeling DO, Webb CH, Cavert W, Wang DH, Brundage RC. A prospective clinical study of Epstein-Barr virus and host interactions during acute infectious mononucleosis. J Infect Dis 2005;192:1505-12. [PubMed]
10. Bar RS, DeLor CJ, Clausen KP, Hurtubise P, Henle W, Hewetson JF. Fatal infectious mononucleosis in a family. N Engl J Med 1974;290:363-7. [PubMed]
11. Bender CE. The value of corticosteroids in the treatment of infectious mononucleosis. JAMA 1967;199:529-31. [PubMed]
12. Benoit L, Wang X, Pabst HF, Dutz J, Tan R. Cutting Edge: Defective NK Cell Activation in X-Linked Lymphoproliferative Disease. J Immunol 2000;165:3549-3553. [PubMed]
13. Chuang HC, Lay JD, Hsieh WC, Wang HC, Chang Y, Chuang SE, Su IJ. Epstein-Barr virus LMP1 inhibits the expression of SAP gene and upregulates Th1 cytokines in the pathogenesis of hemophagocytic syndrome. Blood 2005;106:3090–3096. [PubMed]
14. Chung B, Aoukaty A, Dutz J, Terhorst C, Tan R. Signaling lymphocytic activation molecule-associated protein controls NKT cell functions. J Immunol 2005;174:3153-7. [PubMed]
15. Coffey AJ, Brooksbank RA, Brandau O, Oohashi T, Howell GR, Bye JM, Cahn AP, Durham J, Heath P, Wray P, Pavitt R, Wilkinson J, Leversha M, Huckle E, Shaw-Smith CJ, Dunham A, Rhodes S, Schuster V, Porta G, Yin L, Serafini P, Sylla B, Zollo M, Franco B, Bentley DR, and et al. Host response to EBV infection in X-linked lymphoproliferative disease results from mutations in an SH2-domain encoding gene. Nat Genet 1998;20:129-35. [PubMed]
16. Cohen JI, Jaffe ES, Dale JK, Pittaluga S, Heslop HE, Rooney CM, Gottschalk S, Bollard CM, Rao VK, Marques A, Burbelo PD, Turk SP, Fulton R, Wayne AS,Little RF, Cairo MS, El-Mallawany NK, Fowler D, Sportes C, Bishop MR, Wilson W, Straus SE. Characterization and treatment of chronic active Epstein-Barr virus disease: a 28-year experience in the United States. Blood 2011;117:5835-49. [PubMed]
17. Colby B, Shaw JE, Datta AK, Pagano JS. Replication of Epstein-Barr virus DNA in lymphoblastoid cells treated for extended periods with acyclovir. Am J Med 1982;73:77-81. [PubMed]
18. Colby B, Shaw JE, Elion GB, Pagano JS. Effect of acyclovir [9-(2-hydroxyethoxymethyl)guanine] on Epstein- Barr virus DNA replication. J Virol 1980;34:560-8. [PubMed]
19. Collins M, Fleisher G, Kreisberg J, Fager S. Role of steroids in the treatment of infectious mononucleosis in the ambulatory college student. J Am Coll Health 1984;33:101-5. [PubMed]
20. Condon LM, Cederberg LE, Rabinovitch MD, Liebo RV, Go JC, Delaney AS, Schmeling DO, Thomas W, Balfour HH Jr. Age-specific prevalence of Epstein-Barr virus infection among Minnesota children: effects of race/ethnicity and family environment. Clin Infect Dis 2014;59:501-8. [PubMed]
21. Copeman H. Infectious mononucleosis with severe thrombocytopenic purpura. Med J Aust 1956;43:925-927. [PubMed]
22. Crawford DH, Macsween KF, Higgins CD, Thomas R, McAulay K, Williams H, Harrison N, Reid S, Conacher M, Douglas J, Swerdlow AJ. A cohort study among university students: identification of risk factors for Epstein-Barr virus seroconversion and infectious mononucleosis. Clin Infect Dis 2006;43:276-82.[PubMed]
23. Crawford DH, Swerdlow AJ, Higgins C, McAulay K, Harrison N, Williams H, Britton K, Macsween KF. Sexual history and Epstein-Barr virus infection. J Infect Dis 2002; 186:731-6. [PubMed]
24. De Diego JI, Prim MP, Hardisson D, Verdaguer JM, Jara P. Post-transplant lymphoproliferative disease in tonsils of children with liver transplantation. Int J Pediatr Otorhinolaryngol. 2001; 58: 113-118. [PubMed]
25. Dellemijn P, Brandenburg A, Niesters HG, van den Bent MJ, Rothbarth PH, Vlasveld LT. Successful treatment with ganciclovir of presumed Epstein-Barr meningo-encephalitis following bone marrow transplant. Bone Marrow Transplant 1995;16:311-2. [PubMed]
26. Dommerby H, Stangerup SE, Stangerup M, Hancke S. Hepatosplenomegaly in infectious mononucleosis, assessed by ultrasonic scanning. J Laryngol Otol 1986;100:573-9. [PubMed]
27. Elazary AS, Wolf DG, Amir G, Avni B, Rund D, Yehuda DB, et al. Severe Epstein-Barr virus-associated hemophagocytic syndrome in six adults patients. J Clin Virol 2007;40:156-9. [PubMed]
28. Evans AS, Niederman JC, Cenabre LC, West B, Richards VA. A prospective evaluation of heterophile and Epstein-Barr virus-specific IgM antibody tests in clinical and subclinical infectious mononucleosis: Specificity and sensitivity of the tests and persistence of antibody. J Infect Dis 1975;132:546-54. [PubMed]
29. Faller DV, Mentzer SJ, Perrine SP. Induction of the Epstein-Barr virus thymidine kinase gene with concomitant nucleoside antivirals as a therapeutic strategy for Epstein- Barr virus-associated malignancies. Curr Opin Oncol2001;13:360-7. [PubMed]
30. Farley DR, Zietlow SP, Bannon MP, Farnell MB. Spontaneous rupture of the spleen due to infectious mononucleosis. Mayo Clin Proc1992; 67:846-53. [PubMed]
31. Finch SC. In: Infectious Mononucleosis, Carter, RL, Penman, HG (eds), Blackwell Scientific Publication, Oxford and Ediburgh 1969. pp.47-62.
32. Funch DP, Walker AM, Schneider G, Ziyadeh NJ, Pescovitz MD. Ganciclovir and acyclovir reduce the risk of post-transplant lymphoproliferative disorder in renal transplant recipients. Am J Transplant. 2005; 5: 2894-2900. [PubMed]
33. Gahn B, Siller-Lopez F, Pirooz AD, Yvon E, Gottschalk S, Longnecker R, Brenner MK, Heslop HE, Aguilar-Cordova E, Rooney CM. Adenoviral gene transfer into dendritic cells efficiently amplifies the immune response to LMP2A antigen: a potential treatment strategy for Epstein-Barr virus--positive Hodgkin's lymphoma. Int J Cancer 2001;93:706-13. [PubMed]
34. Giron-Michel J, Menard F, Negrini S, Devocelle A, Azzarone B, Besson C. EBV-associated mononucleosis does not induce long-term global deficit in T-cell responsiveness to IL-15. Blood. 2009;113:4541-7. [PubMed]
35.Gottschalk S, Ng CY, Perez M, Smith CA, Sample C, Brenner MK, Heslop HE, Rooney CM. An Epstein-Barr virus deletion mutant associated with fatal lymphoproliferative disease unresponsive to therapy with virus-specific CTLs. Blood 2001;97:835-43. [PubMed]
36. Gottschalk S, Rooney CM, Heslop HE. Post-transplant lymphoproliferative disorders. Ann Rev Med 2005; 56:29-44. [PubMed]
37. Green M. Management of Epstein-Barr virus-induced post-transplant lymphoproliferative disease in recipients of solid organ transplantation. Am J Transplant. 2001;1:103-108. [PubMed]
38. Greenspan JS, Greenspan D, Lennette ET, Abrams DI, Conant MA, V. Petersen V, Freese UK. Replication of Epstein-Barr virus within the epithelial cells of oral "hairy" leukoplakia, an AIDS-associated lesion. N Engl J Med1985; 313:1564-71. [PubMed]
39. Gross TG, Filipovich AH, Conley ME, Pracher E, Schmiegelow K, Verdirame JD, Vowels M, Williams LL, Seemayer TA. Cure of X-linked lymphoproliferative disease (XLP) with allogeneic hematopoietic stem cell transplantation (HSCT): report from the XLP registry. Bone Marrow Transplant 1996;17:741-4. [PubMed]
40. Gu S, Huang TM, Ruan L, Miao YH, Lu H, Chu CM, Motz M, Wolf H. First EBV vaccine trial in humans using recombinant vaccinia virus expressing the major membrane antigen. Dev Biol Stand 1995; 84:171-7. [PubMed]
41. Guthery SL, Heubi JE, Bucuvalas JC, Gross TG, Ryckman FC, Alonso MH, Balistreri WF, Hornung RW. Determination of risk factors for Epstein-Barr virus-associated posttransplant lymphoproliferative disorder in pediatric liver transplant recipients using objective case ascertainment. Transplantation. 2003;75:987-993. [PubMed]
42. Hal SV, Senanayake, S, Hardiman, R. Splenic infarction due to transient antiphospholipid antibodies induced by acute Epstein-Barr virus infection. J Clin Virol 2005; 32:245-7. [PubMed]
43. Hanto D, Gajl-Peczalska KJ, Frizzera G, Arthur DC, Balfour HH, Jr., McClain K, Simmons RL, Najarian JS. Epstein-Barr virus (EBV) induced polyclonal and monoclonal B-cell lymphoproliferative diseases occurring after renal transplantation. Clinical, pathologic, and virologic findings and implications for therapy. Ann Surg1983:198. [PubMed]
44. Hanto DW, Frizzera G, Gajl-Peczalska J, Purtilo DT, Klein G, Simmons RL, Najarian JS. The Epstein-Barr Virus (EBV) In the Pathogenesis Of Posttransplant Lymphoma. Transplant Proc 1981;13:756-60. [PubMed]
45. Hanto DW, Gajl-Peczalska KJ, Sakamoto K, Purtilo DT, Balfour HH, Simmons RL, Najarian JS. Epstein-Barr Virus-Induced B-Cell Lymphoma After Renal Transplantation: Acyclovir Therapy and Transition From Polyclonal to Monoclonal B-Cell Proliferation. N Engl J Med1982; 306:913-918. [PubMed]
46. Helminen M, Fau-Lahdenpohja N, Lahdenpohja M, Fau-Hurme N, Hurme M. Polymorphism of the interleukin-10 gene is associated with susceptibility to Epstein-Barr virus infection. J Infect Dis 1991;180:496-499. [PubMed]
47. Henle G, Henle W. Observations on childhood infections with the Epstein-Barr virus. J Infect Dis1970;121:303-10.[PubMed]
48. Henle G, Henle W, Clifford P, DiehlV, Kafuko GW, Kirya BG, Klein G, Morrow RH, Munube GM, Pike P, Tukei PM, Ziegler JL. Antibodies to Epstein-Barr virus in Burkitt's lymphoma and control groups. J Natl Cancer Inst 1969;43:1147-57. [PubMed]
49. Henie G, Henle W, Horwitz CA. Antibodies to Epstein-Barr virus-associated nuclear antigen in infectious mononucleosis. J Infect Dis 1974;130:231-9.[PubMed]
50. Henter JI, Horne A, Arico M, Egeler RM. Filipovich AH, Imashuku S, et al. HLH-2004: Diagnostic and therapeutic guildelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer 2007;48:124-31. [PubMed]
51. Heslop HE, Perez M, Benaim E, Rochester R, Brenner MK, Rooney CM. Transfer of EBV-specific CTL to prevent EBV lymphoma post bone marrow transplant. J Clin Apheresis1999;14:154-6. [PubMed]
52. Heslop HE, Slobod KS, Pule MA, Hale GA, Rousseau A, Smith CA, Bollard CM, Liu H, Wu MF, Rochester RJ, Amrolia PJ, Hurwitz JL, Brenner MK, Rooney CM. Long-term outcome of EBV-specific T-cell infusions to prevent or treat EBV-related lymphoproliferative disease in transplant recipients. Blood. 2010;4;115:925-35. [PubMed]
53. Hjalgrim H, Askling J, Rostgaard K, Hamilton-Dutoit S, Frisch M, Zhang JS, Madsen M, Rosdahl N, Konradsen HB, Storm HH, Melbye M. Characteristics of Hodgkin's lymphoma after infectious mononucleosis. N Engl J Med 2003;349:1324-32. [PubMed]
54. Hoagland RJ. Infectious mononucleosis. Prim Care 1975;2:295-307. [PubMed]
55. Holmes G, Kaplan JE, Stewart JA, Hunt B, Pinsky PF, Schonberger LB. A cluster of patients with a chronic mononucleosis-like syndrome. Is Epstein-Barr virus the cause? JAMA 1987:257. [PubMed]
56. Horwitz C, Henle W, Henle G, Rudnick H, Latts E. Long-term serological follow-up of patients for Epstein-Barr virus after recovery from infectious mononucleosis. J Infect Dis 1985:151. [PubMed]
57. Hsu JL, Glaser SL. Epstein-barr virus-associated malignancies: epidemiologic patterns and etiologic implications. Crit Rev Oncol Hematol 2000; 34:27-53. [PubMed]
58. Huck K, Feyen O, Niehues T, Ruschendorf F, Hubner N, Laws HJ, Telieps T, Knapp S, Wacker HH, Meindl A, Jumaa H, Borkhardt A. Girls homozygous for an IL-2-inducible T cell kinase mutation that leads to protein deficiency develop fatal EBV-associated lymphoproliferation. The Journal of clinical investigation 2009;119:1350-8. [PubMed]
59. Humar A, Hébert D, Davies HD, Humar A, Stephens D, O'Doherty B, Allen U. A randomized trial of ganciclovir versus ganciclovir plus immune globulin for prophylaxis against Epstein-Barr virus related posttransplant lymphoproliferative disorder. Transplantation. 2006;81:856-861. [PubMed]
60. Ishida Y, Yokota Y, Tauchi H, Fukuda M, Takaoka T, Hayashi M, Matsuda H. Ganciclovir for chronic active Epstein-Barr virus infection. Lancet 1993:341.[PubMed]
61. Israele V, Shirley P, Sixbey JW. Excretion of the Epstein-Barr virus from the genital tract of men. J Infect Dis 1991;163:1341-3. [PubMed]
62. Jia, WH, Collins A, Zeng YX, Feng BJ, Yu XJ, Huang LX, Feng QS, Huang P, Yao MH, Shugart YY. Complex segregation analysis of nasopharyngeal carcinoma in Guangdong, China: evidence for a multifactorial mode of inheritance (complex segregation analysis of NPC in China). Eur J Hum Genet 2004;13:248-252. [PubMed]
63. Kaplan LD, Lee JY, Ambinder RF, Sparano JA, Cesarman E, Chadburn A, Levine AM, Scadden DT. Rituximab does not improve clinical outcome in a randomized phase 3 trial of CHOP with or without rituximab in patients with HIV-associated non-Hodgkin lymphoma: AIDS-Malignancies Consortium Trial 010. Blood. 2005;106:1538-1543. [PubMed]
64. Katano H, Ali MA, Patera AC, Catalfamo M, Jaffe ES, Kimura H, Dale JK, Straus SE, Cohen JI. Chronic active Epstein-Barr virus infection associated with mutations in perforin that impair its maturation. Blood 2004;103:1244-52. [PubMed]
65. Kawa KT. Okamura K, Yagi M, Takeuchi M, Nakayama, Inoue M. Mosquito allergy and Epstein-Barr virus-associated T/natural killer- cell lymphoproliferative disease. Blood 2001; 98:3173-4. [PubMed]
66. Kedes DH, Ganem D. Sensitivity of Kaposi's sarcoma-associated herpesvirus replication to antiviral drugs. Implications for potential therapy. J Clin Invest 1997; 99:2082-6. [PubMed]
67. Kennedy G, Komano J, Sugden B. Epstein-Barr virus provides a survival factor to Burkitt's lymphomas. PNAS 2003;100:14269-14274. [PubMed]
68. Khanna R, Moss DJ, Burrows SR. Vaccine strategies against EBVassociated diseases: lessons from studies on cytotoxic T-cell mediated immune regulation. Immunological Rev 1999;170:49-64. [PubMed]
69. Kimura H, Hoshino Y, Kanegane H, Tsuge I, Okamura T, Kawa K, Morishima T. Clinical and virologic characteristics of chronic active Epstein-Barr virus infection. Blood 2001;98:280-6. [PubMed]
70. Kimura H, Ito Y, Kawabe S, Gotoh K, Takahashi Y, Kojima S, Naoe T, Esaki S, Kikuta A, Sawada A, Kawa K, Ohshima K, Nakamura S. Epstein-Barr virus (EBV)-associated T/NK lymphoproliferative diseases in non-immunocompromised hosts: prospective analysis of 108 cases. Blood 2011;119:673-86. [PubMed]
71. Kimura H, Morita M, Yabuta Y, Kuzushima K, Kato K, Kojima S, Matsuyama T, Morishima T. Quantitative analysis of Epstein-Barr virus load by using a real-time PCR assay. J Clin Microbiol 1999;37:132-136. [PubMed]
72. Klein E, Cochran JF, Buck RL. The effects of short-term corticosteroid therapy on the symptoms of infectious mononucleosis pharyngotonsillitis: a double-blind study. J Am Coll Health Assoc 1969;17:446-52. [PubMed]
73. Kuehnle I, Huls MH, Liu Z, Semmelmann M, Krance RA, Brenner MK, Rooney CM, Heslop HE. CD20 monoclonal antibody (rituximab) for therapy of Epstein-Barr virus lymphoma after hemopoietic stem-cell transplantation. Blood 2000; 95:1502-5. [PubMed]
74. Lahat E, Berkoritch M, Barr J, et al. Abnormal visual evoked potentials in children with "Alice in Wonderland" syndrome due to infectious mononucleosis. J Child Neurol 1999;44:732-5. [PubMed]
75. Landgren O, Gilbert ES, Rizzo JD, et al. Risk factors for lymphoproliferative disorders after allogeneic hematopoietic cell transplantation. Blood. 2009; 113: 4992-5001. [PubMed]
76. Latour S, Aguilar C. XIAP deficiency syndrome in humans. Semin Cell Dev Biol. 2015;39:115-123. [PubMed]
77. LeClaire AC, Martin CA, Hoven AD. Rash associated with piperacillin/tazobactam administration in infectious mononucleosis. Ann Pharmacother 2004;38:996-8. [PubMed]
78. Li FY, Chaigne-Delalande B, Su H, Uzel G, Matthews H, Lenardo MJ. XMEN disease: a new primary immunodeficiency affecting Mg2+ regulation of immunity against Epstein-Barr virus. Blood 2014;123:2148-52. [PubMed]
79. Lin J, Smith MC, Pagano JS. Prolonged inhibitory effect of 9-(1,3-dihydroxy-2- propoxymethyl)guanine against replication of Epstein-Barr virus. J Virol 1984:50. [PubMed]
80. Little RF, Pittaluga S, Grant N, Steinberg SM, Kavlick MF, Mitsuya H, Franchini G, Gutierrez M, Raffeld M, Jaffe ES, Shearer G, Yarchoan R, Wilson WH. Highly effective treatment of acquired immunodeficiency syndrome-related lymphoma with dose-adjusted EPOCH: impact of antiretroviral therapy suspension and tumor biology. Blood 2003;101:4653-9. [PubMed]
81. Littler E, McBride ZJ, Trost AA, Sorensen E, Powell KL, Walsh-Arrand JE, Arrand JR. Identification of an Epstein-Barr virus-coded thymidine kinase. EMBO J 1986;5:1959-66 [PubMed]
82. Longnecker R, Kieff E, Cohen J. Epstein-Barr Virus. In: Knipe DM, Howley PM, editors. Fields Virology. 5 ed. Philadelphia: Lippincott Williams and Wilkins, 2013:1898-959.
83. Machado AS, Apa AG, Magalhães de Rezende LM, et al. Plasma Epstein-Barr viral load predicting response after chemotherapy for post-transplant lymphoproliferative disease. Clin Exp Med. 2008; 8: 129-132. [PubMed]
84. McAulay KA, Haque T, Crawford DH. Tumour necrosis factor gene polymorphism: a predictive factor for the development of post-transplant lymphoproliferative disease. Br J Cancer. 2009; 101:1019-1027. [PubMed]
85. McCloskey GL, Massa MC. Cephalexin rash in infectious mononucleosis. Cutis 1997;59:251-4. [PubMed]
86. McGowan J, Jr., Chesney PJ, Crossley KB, LaForce FM. Guidelines for the use of systemic glucocorticosteroids in the management of selected infections. Working Group on Steroid Use, Antimicrobial Agents Committee, Infectious Diseases Society of America. J Infect Dis 1992;165:1-13. [PubMed]
87. Meng Q, Hagemeier SR, Fingeroth JD, Gershburg E, Pagano JS, Kenney SC. The Epstein-Barr virus (EBV)-encoded protein kinase, EBV-PK, but not the thymidine kinase (EBV-TK), is required for ganciclovir and acyclovir inhibition of lytic viral production. J Virol 2010;84:4534-42. [PubMed]
88. Mentzer SJ, Perrine SP, Faller DV. Epstein--Barr virus post-transplant lymphoproliferative disease and virus-specific therapy: pharmacological re-activation of viral target genes with arginine butyrate. Transpl Infect Dis (Sweden), 2001;3(3):177-85. [PubMed]
89. Migliorati CA, Jones AC, Baughman PA. Use of exfoliative cytology in the diagnosis of oral hairy leukoplakia. Oral Surg Oral Med Oral Pathol. 1993; 76: 704-710. [PubMed]
90. Miller G, Grogan E, Rowe D, Rooney C, Heston L, Eastman R, Andiman W, Niederman J, Lenoir G, Henle W, Sullivan J, Schooley R, Vossen J, Strauss S, Issekutz T. Selective lack of antibody to a component of EB nuclear antigen in patients with chronic active Epstein-Barr virus infection. J Infect Dis 1987; 156:26-35. [PubMed]
91. Moghaddam A, RM, Lee-Parritz D, Annis B, Johnson RP, Wang F. An animal model for acute and persistent Epstein-Barr virus infection. Science 1997;276:2030-3. [PubMed]
92. Morgan A, Finerty S, Lovgren K, Scullion FT, Morein B. Prevention of Epstein-Barr (EB) virus-induced lymphoma in cottontop tamarins by vaccination with the EB virus envelope glycoprotein gp340 incorporated into immune-stimulating complexes. J Gen Virol 1988; 69:2093-6. [PubMed]
93. Morgan A, Mackett M, Finerty S, Arrand JR, Scullion FT, Epstein MA. Recombinant vaccinia virus expressing Epstein-Barr virus glycoprotein gp340 protects cottontop tamarins against EB virus-induced malignant lymphomas. J Med Virol 1988;25:189-95. [PubMed]
94. Morgan A, Wilson DA. Epstein-Barr Virus Gp350 Vaccines. Epstein-Barr Virus Report 1997;4:33-39. [PubMed]
95. Morton LM, Wang SS, Devesa SS, Hartge P, Weisenburger DD, Linet MS. Lymphoma incidence patterns by WHO subtype in the United States, 1992-2001. Blood 2006;107:265-276. [PubMed]
96. Mosialos G, Birkenbach M, Yalamanchili R, VanArsdale T, Ware C, Kieff E. The Epstein-Barr virus transforming protein LMP1 engages signaling proteins for the tumor necrosis factor receptor family. Cell 1995; 80:389-99. [PubMed]
97. Nakatsuka S, Yao M, Hoshida Y, Yamamoto S, Iuchi K, Aozasa K. Pyothorax-associated lymphoma: a review of 106 cases. J Clin Oncol 2002;20:4255-60. [PubMed]
98. Nemerow GR, Mold C, Schwend VK, Tollefson V, Cooper NR. Identification of gp350 as the viral glycoprotein mediating attachment of Epstein-Barr virus (EBV) to the EBV/C3d receptor of B cells: sequence homology of gp350 and C3 complement fragment C3d. J Virol 1987;61:1416-20. [PubMed]
99. Nichols KE, Hom J, Gong S-Y, Ganguly A, Ma CS, Cannons JL, Tangye SG, Schwartzberg PL, Koretzky GA, Stein PL. Regulation of NKT cell development by SAP, the protein defective in XLP. Nat Med 2005; 11:340-345. [PubMed]
100. Niederman JC, Evans AS, Subrahmanyan L, McCollum RW. Prevalence, incidence and persistence of EB virus antibody in young adults. N Engl J Med 1970;282:361-5. [PubMed]
101. Oettle H, Wilborn F, Schmidt CA, Siegert W. Treatment with ganciclovir and Ig for acute Epstein-Barr virus infection after allogeneic bone marrow transplantation. Blood 1993;82:2257-8. [PubMed]
102. Ok CY, Papathomas TG, Medeiros LJ, Young KH. EBV-positive diffuse large B-cell lymphoma of the elderly. Blood 2013;122:328-40. [PubMed]
103. Pagano J, Datta AK. Perspectives on interactions of acyclovir with Epstein-Barr and other herpes viruses. Am J Med 1982;73:18-26. [PubMed]
104. Pagano J, Sixbey JW, Lin JC. Acyclovir and Epstein-Barr virus infection. J Antimicrob Chemother 1983;12:113-21. [PubMed]
105. Paily R. Quinolone drug rash in a patient with infectious mononucleosis. J Dermatol 2000; 27:405-6. [PubMed]
106. Parkin DM, Muir CS. Cancer Incidence in Five Continents. Comparability and quality of data. IARC Sci Publ 1992:45-173. [PubMed]
107. Pasquier B, Yin L, Fondaneche MC, Relouzat F, Bloch-Queyrat C, Lambert N, Fischer A, de Saint-Basile G, Latour S. Defective NKT cell development in mice and humans lacking the adapter SAP, the X-linked lymphoproliferative syndrome gene product. J Exper Med 2005;201:695-701. [PubMed]
108. Pitetti RD, Laus S, Wadowsky RM. Clinical evaluation of a quantitative real time polymerase chain reaction assay for diagnosis of primary Epstein-Barr virus infection in children. Pediatr Infect Dis J 2003; 22:736-739. [PubMed]
109. Polesel J, Clifford GM, Rickenbach M, et al. Non-Hodgkin lymphoma incidence in the Swiss HIV Cohort Study before and after highly active antiretroviral therapy. AIDS. 2008; 22: 301-306. [PubMed]
110. Porter DD, Wimberly I, Benyesh-Melnick M. Prevalence of antibodies to EB virus and other herpesviruses. Jama 1969;208:1675-9. [PubMed]
111. Preiksaitis JK. New developments in the diagnosis and management of posttransplantation lymphoproliferative disorders in solid organ transplant recipients. Clin Infect Dis. 2004; 39: 1016-1023. [PubMed]
112. Preiksaitis JK, Pang XL, Fox JD, Fenton JM, Caliendo AM, Miller GG; American Society of Transplantation Infectious Diseases Community of Practice. Interlaboratory comparison of epstein-barr virus viral load assays. Am J Transplant. 2009; 9: 269-279. [PubMed]
113. Prout C, Dalrymple W. A double-blind study of eighty-two cases of infectious mononucleosis treated with corticosteroids. J Am Coll Health Assoc 1966;15:62-6. [PubMed]
114. Purtilo DT, Cassel CK, Yang JP, Harper R. X-linked recessive progressive combined variable immunodeficiency (Duncan's disease). Lancet 1975;1:935-40.[PubMed]
115. Quintanilla-Martinez L, Ridaura C, Nagl F, Saez-de-Ocariz M, Duran-McKinster C, Ruiz-Maldonado R, Ruiz-Maldonado R, Alderete G, Grube P, Lome-Maldonado C, Bonzheim I, Fend F.Hydroa vacciniforme-like lymphoma: a chronic EBV+ lymphoproliferative disorder with risk to develop a systemic lymphoma. Blood 2013;122:3101-10. [PubMed]
116. Ragot T, Finerty S, Watkins PE, Perricaudet M, Morgan AJ. Replication-defective recombinant adenovirus expressing the Epstein- Barr virus (EBV) envelope glycoprotein gp340/220 induces protective immunity against EBV-induced lymphomas in the cottontop tamarin. J Gen Virol 1993;74:501-7. [PubMed]
117. Ramírez-Amador V, Esquivel-Pedraza L, Sierra-Madero J, et al. The Changing Clinical Spectrum of Human Immunodeficiency Virus (HIV)-Related Oral Lesions in 1,000 Consecutive Patients: A 12-Year Study in a Referral Center in Mexico. Medicine (Baltimore). 2003; 82: 39-50. [PubMed]
118. Rea TD, Russo JE, Katon W, Ashley RL, Buchwald DS. Prospective study of the natural history of infectious mononucleosis caused by Epstein-Barr virus. J Am Board Fam Pract 2001;14:234-42. [PubMed]
119. Resnick L, Herbst JS, Ablashi DV, Atherton S, Frank B, Rosen L, Horwitz SN. Regression of oral hairy leukoplakia after orally administered acyclovir therapy. JAMA 1988;259:384-8. [PubMed]
120. Ribera JM, Oriol A, Morgades M, Gonzalez-Barca E, Miralles P, Lopez-Guillermo A, García M, Pethema Geltamo, Gelcab and Gesida Groups. Safety and efficacy of cyclophosphamide, adriamycin, vincristine, prednisone and rituximab in patients with human immunodeficiency virus-associated diffuse large B-cell lymphoma: results of a phase II trial. Brit J Hematol 2008;140:411-9. [PubMed]
121. Rickinson A, Kieff E. Epstein Barr virus p. 2575-2627. In D. Knipe and P. Howley (ed.), Fields Virology, 3 ed, vol. 2. Lippincott Williams, Philadelphia, 2001. [PubMed]
122. Rickinson A, Kieff E. Epstein Barr virus and its replication, p. 2511-2573. In D. Knipe and P. Howley (ed.), Fields Virology, 3 ed, vol. 2. Lippincott Williams, Philadelphia, 2001. [PubMed]
123. Rivailler P, Jiang H, Cho Yg, Quink C, Wang F. Complete Nucleotide Sequence of the Rhesus Lymphocryptovirus: Genetic Validation for an Epstein-Barr Virus Animal Model. J Virol 2002;76:421-426. [PubMed]
124. Rooney C, Smith CA, Ng CY, Loftin S, Li C, Krance RA, Brenner MK, Heslop HE. Use of gene-modified virus-specific T lymphocytes to control Epstein- Barr-virus-related lymphoproliferation. Lancet 1995; 345:9-13. [PubMed]
125. Rooney CM, Smith CA, Ng CY, Loftin SK, Sixbey JW, Gan Y, Srivastava DK, Bowman LC, Krance RA, Brenner MK, Heslop HE. Infusion of cytotoxic T cells for the prevention and treatment of Epstein-Barr virus-induced lymphoma in allogeneic transplant recipients. Blood 1998; 92:1549-55. [PubMed]
126. Rostgaard K, Wohlfahrt J, Hjalgrim H. A genetic basis for infectious mononucleosis: evidence from a family study of hospitalized cases in Denmark. Clin Infect Dis 2014;58:1684-9. [PubMed]
127. Sauce D, Larsen M, Curnow SJ, Leese AM, Moss PA, Hislop AD, Salmon M, Rickinson AB. EBV-associated mononucleosis leads to long-term global deficit in T-cell responsiveness to IL-15. Blood 2006;108:11-8. [PubMed]
128. Savoldo B, Heslop HE, Rooney CM. The use of cytotoxic t cells for the prevention and treatment of epstein-barr virus induced lymphoma in transplant recipients. Leuk Lymphoma 2000; 39:455-64. [PubMed]
129. Sawyer RN, Evans AS, Niederman JC, McCollum RW. Prospective studies of a group of Yale University freshmen. I. Occurrence of infectious mononucleosis. J Infect Dis 1971;123:263-70. [PubMed]
130. Schissel DJ, Singer D, David-Bajar K. Azithromycin eruption in infectious mononucleosis: a proposed mechanism of interaction. Cutis 2000; 65:163-166.[PubMed]
131. Schooley R, Carey RW, Miller G, Henle W, Eastman R, Mark EJ, Kenyon K, Wheeler EO, Rubin RH. Chronic Epstein-Barr virus infection associated with fever and interstitial pneumonitis: Clinical and serologic features and response to antiviral chemotherapy. Ann Intern Med 1986;104:636-43. [PubMed]
132. Schumacher H, Jacobson W, Bemiller C. Treatment of infectious mononucleosis. Ann Intern Med 1963;58. [PubMed]
133. Sebelin-Wulf K, Nguyen TD, Oertel S, et al. Quantitative analysis of EBV-specific CD4/CD8 T cell numbers, absolute CD4/CD8 T cell numbers and EBV load in solid organ transplant recipients with PLTD. Transpl Immunol. 2007; 17: 203-210. [PubMed]
134. Shiboski CH, Patton LL, Webster-Cyriaque JY, et al. The Oral HIV/AIDS Research Alliance: updated case definitions of oral disease endpoints. J Oral Pathol Med. 2009; 38:481-488. [PubMed]
135. Sixbey JW, Lemon SM, Pagano JS. A second site for Epstein-Barr virus shedding: the uterine cervix. Lancet 1986;2(8516):1122-4. [PubMed]
136. Stevens SJ, Verkuijlen SA, Hariwiyanto B, Harijadi, Paramita DK, Fachiroh J, Adham M, Tan IB, Haryana SM, Middeldorp JM. Noninvasive diagnosis of nasopharyngeal carcinoma: Nasopharyngeal brushings reveal high Epstein-Barr virus DNA load and carcinoma-specific viral BARF1 mRNA. International Journal of Cancer 2006;119:608-614. [PubMed]
137. Smith J. Complications of infectious monucleosis. Ann Intern Med 1956;44:861-873. [PubMed]
138. Sokal EM, Hoppenbrouwers K, Vandermeulen C, et al. Recombinant gp350 vaccine for infectious mononucleosis: a phase 2, randomized, double-blind, placebo-controlled trial to evaluate the safety, immunogenicity, and efficacy of an Epstein-Barr virus vaccine in healthy young adults. J Infect Dis (United States), 2007:196:1749-53. [PubMed]
139. Song JY, Pittaluga S, Dunleavy K, Grant N, White T, Jiang L, Davies-Hill T, Raffeld M, Wilson WH, Jaffe ES. Lymphomatoid granulomatosis--a single institute experience: pathologic findings and clinical correlations. Amer J Surg Pathol 2015;39:141-56. [PubMed]
140. Starzl T, Nalesnik MA, Porter KA, Ho M, Iwatsuki S, Griffith BP, Rosenthal JT, Hakala TR, Shaw BW, Jr., Hardesty RL, Atchison RW, Jaffe R, Bahnson HT. Reversibility of lymphomas and lymphoproliferative lesions developing under cyclosporin-steroid therapy. Lancet 1984;1:583-7. [PubMed]
141. Stepp SE, Dufourcq-Lagelouse R, Le Deist F, Bhawan S, Certain S, Mathew PA, Henter JI, Bennett M, Fischer A, de Saint Basile G, Kumar V. Perforin gene defects in familial hemophagocytic lymphohistiocytosis. Science 1999;286(5446):1957-9. [PubMed]
142. Straus S. The chronic mononucleosis syndrome. J Infect Dis 1988:157:405-412. [PubMed]
143. Straus S, Cohen JI, Tosato G, Meier J. NIH conference. Epstein-Barr virus infections: biology, pathogenesis, and management. Ann Intern Med 1993;118:45-58. [PubMed]
144. Straus S, Dale JK, Tobi M, Lawley T, Preble O, Blaese RM, Hallahan C, Henle W. Acyclovir treatment of the chronic fatigue syndrome. Lack of efficacy in a placebo-controlled trial. N Engl J Med 1988:319. [PubMed]
145. Styczynski J, Einsele H, Gil L, Ljungman P. Outcome of treatment of Epstein-Barr virus-related post-transplant lymphoproliferative disorder in hematopoietic stem cell recipients: a comprehensive review of reported cases. Transpl Infect Dis. 2009;11(5):383-92. [PubMed]
146. Su IJ, Chen RL, Lin DT, Lin KS, Chen CC. Epstein-Barr virus (EBV) infects T lymphocytes in childhood EBV-associated hemophagocytic syndrome in Taiwan. Am J Pathol 1994;144:1219–1225 [PubMed]
147. Subar M, Neri A, Inghirami G, et al. Frequent c-myc oncogene activation and infrequent presence of Epstein-Barr virus genome in AIDS-associated lymphoma. Blood (United States), 1988;72:667-71. [PubMed]
148. Sullivan JL, Woda BA, Herrod HG, et al. Epstein-Barr virus associated hemophagocytic syndrome: Virological and immunopathological studies. Blood 1985;65:65:1097-104. [PubMed]
149. Tsai DE, Douglas L, Andreadis C, et al. EBV PCR in the diagnosis and monitoring of posttransplant lymphoproliferative disorder: results of a two-arm prospective trial. Am J Transplant. 2008;8:1016-1024. [PubMed]
150. Tsai DE, Hardy CL, et al. "Reduction in immunosuppression as initial therapy for posttransplant lymphoproliferative disorder: analysis of prognostic variables and long-term follow-up of 42 adult patients." Transplantation 2001;71:1076-88.
151. Tselis A, Duman R, Storch GA, Lisak RP. Epstein-Barr virus encephalomyelitis diagnosed by polymerase chain reaction: Detection of the genome in the CSF. Neurology 1997;48:1351-5. [PubMed]
152.Torre D, Tambini R. Acyclovir for treatment of infectious mononucleosis: a meta-analysis. Scand J Infect Dis 1999;31:543-7. [PubMed]
153. Tynell E, Aurelius E, Brandell A, Julander I, Wood M, Yao QY, Rickinson A, Akerlund B, Andersson J. Acyclovir and prednisolone treatment of acute infectious mononucleosis: a multicenter, double-blind, placebo-controlled study. J Infect Dis 1996;174:324-31. [PubMed]
154. van der Horst C, Joncas J, Ahronheim G, Gustafson N, Stein G, Gurwith M, Fleisher G, Sullivan J, Sixbey J, Roland S, Fryer J, Champney K, Schooley R, Sumaya C, Pagano J. Lack of effect of peroral acyclovir for the treatment of acute infectious mononucleosis. J Infect Dis. 1991;164:788-792 [PubMed]
155. Vetsika EK, Callan M. Infectious mononucleosis and Epstein-Barr virus. Expert Rev Mol Med. 2004;6:1-16. [PubMed]
156. Vokes EE, Liebowitz DN, Weichselbaum RR. Nasopharyngeal carcinoma. Lancet. 1997; 350: 1087-91. [PubMed]
157. Waldo R. Neurologic complications of infectious mononucleosis after steroid therapy. South Med J 1981;74:1159-1160. [PubMed]
158. Weinberger, B, Plentz, A, Weinberger, KM, et al. Quantitation of Epstein-Barr virus mRNA using reverse transcription and real-time PCR. J Med Virol 2004;74:612-618. [PubMed]
159. Weinstock DM, Ambrossi GG, Brennan C, Kiehn TE, Jakubowski A. Preemptive diagnosis and treatment of Epstein-Barr virus-associated post transplant lymphoproliferative disorder after hematopoietic stem cell transplant: an approach in development. Bone Marrow Transplant. 2006;37:539-546. [PubMed]
160. Xicoy B, Ribera JM, Muller M, Garcia O, Hoffmann C, Oriol A, Hentrich M, Grande C, Wasmuth JC, Esteve J, van Lunzen J, Del Potro E, Knechten H, Brunet S, Mayr C, Escoda L, Schommers P, Alonso N, Vall-Llovera F, Pérez M, Morgades M, González J, Fernández A, Thoden J, Gökbuget N, Hoelzer D, Fätkenheuer G,Wyen C; PETHEMA Group and German HIV Lymphoma Cohort. Dose-intensive chemotherapy including rituximab is highly effective but toxic in human immunodeficiency virus-infected patients with Burkitt lymphoma/leukemia: parallel study of 81 patients. Leuk Lymphoma 2014;55:2341-8. [PubMed]
161. Yao Q, Ogan P, Rowe M, Wood M, Rickinson AB. The Epstein-Barr virus host balance in acute infectious mononucleosis patients receiving acyclovir anti-viral therapy. Int J Cancer 1989;43:61-66. [PubMed]
162. Yu MC, Ho JH, Lai SH, Henderson BE. Cantonese-style salted fish as a cause of nasopharyngeal carcinoma: report of a case-control study in Hong Kong. Cancer Res 1986;46:956-961. [PubMed]
163. Zou P, Kawada J, Pesnicak L, et al. Bortezomib induces apoptosis of Epstein-Barr virus (EBV)-transformed B cells and prolongs survival of mice inoculated with EBV-transformed B cells. J Virol 2007;81:10029-36 [PubMed]
Tables
Table 1. Typical Patterns of Test Results of Serologic Testing for EBV During Various Stages of Infection.
| Clinical Status | VCA IgM Ab | EA Ab | VCA IgG Ab | EBNA Ab |
|---|---|---|---|---|
| Susceptible | - |
- |
- |
- |
| Acute Infection | + |
+ |
+ |
- |
| Early Convalescence | + |
+ |
+ |
+ |
| Late Convalescence | - |
+ |
+ |
+ |
| Previous Infection | - |
+ (low but fluctuates) |
+ |
+ |
Figure 1. Schematic Representation of the Evolution of Antibodies to Various Epstein-Barr Virus Antigens in Patients with Infectious Mononucleosis.
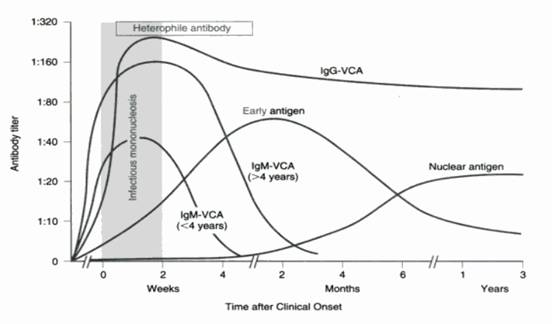
Adopted from 2009 Red Book: Report of the Committee on Infectious Diseases. 28th ed. 2009:291
Figure 2. Change in the Virus Load in a Patient with Infectious Mononucleosis. Sequential samples from a patient with IM were obtained, and both the peripheral blood mononuclear cells (PBMNC) and plasma were analyzed by the real-time PCR assay. The EBV DNA copy numbers are shown per microgram of DNA. The EBV DNA copy numbers are shown per milliliter of plasma. The dotted line shows the detection limit for each sample.
Adopted from Kimura, et al. J Clin Microbiol 1999;37:134.
What's New
Katz BZ, Shiraishi Y, et al. Chronic Fatigue Syndrome After Infectious Mononucleosis in Adolescents. Pediatrics. 2009 Jul;124:189-93.
Hurt C, et al. Diagnostic Evaluation of Mononucleosis-Like Illnesses. Am J Med 2007;120:911.e1-8.
GUIDED MEDLINE SEARCH FOR
Reviews
Hutt-Fletcher L. Epstein-Barr Virus: Cell Trafficking Is Crucial for Persistence. Microbe 2014;9:245-249.
Manuel O, Humar A. EBV-Associated Post-Transplant Lymphoproliferative Diseases in Transplant Recipients.
Adhikari P, Mietzner T. Cell Mediated Immunity.
Styczynski J, et al. Response to Rituximab-Based Therapy and Risk Factor Analysis in Epstein Barr Virus–Related Lymphoproliferative Disorder After Hematopoietic Stem Cell Transplant in Children and Adults: A Study From the Infectious DiseasesWorking Party of the European Group for Blood and Marrow Transplantation. Clin Infect Dis 2013;57:794.
Gulley L, et al. Using Epstein-Barr Viral Load Assays to Diagnose, Monitor, and Prevent Posttransplant Lymphoproliferative Disease. Clin Microb Rev 2010;23:350-366.
Heslop HE. How I treat EBG lymphoproliferation. Blood 2009;114 (19):4002-4008.
Sun HY, et al. Pharmacotherapy of post-transplant viral infections. Expert Opin Pharmacother 2008;9(14):2409-2421.
Funk GA, et al. Viral dynamics in transplant patients: implications for disease. Lancet Infectious Diseases 2007;7:460-472.
Mege JL, Meghari S, Honstettre A, Capo C, Raoult D. The Two faces of interleukin 10 in human infectious diseases. Lancet Infectious Diseases 2006:7;557-569.
Macsween KF, Crawford DH. Epstein-Barr virus-recent advances. Lancet Infect Dis. 2003 Mar;3:131-40.
GUIDED MEDLINE SEARCH FOR RECENT REVIEWS
History
Epstein A. Burkitt lymphoma and the discovery of Epstein-Barr virus. Br J Haematol 2012;156:777-779.
GUIDED MEDLINE SEARCH FOR HISTORICAL ASPECTS
Table of Contents
- Virology
- Epidemiology
- Clincal Manifestations
- Laboratory Diagnosis
- Pathogenesis
- Susceptiblity in Vitro and in Vivo
- Antiviral Therapy
- Adjunctive Therapy
- Vaccines
- References